
Rawpixel.com/shutterstock.com
The Medical Decision Making (MDM) of an evaluation and management (E/M) visit is one of the three components of determining the level of a patient’s visit. But the MDM can sometimes be the most difficult component, as this is where the provider’s thought process is quantified in deciding the correct level of E/M service. In the American Medical Association Current Procedural Terminology (CPT) manual, the level of complexity of MDM is considered to be a function of three variables, which are also reflected in the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines for Evaluation and Management Services:
- The number of possible diagnoses and/or the number of management options that must be considered;
- The amount and/or complexity of medical records, diagnostic tests and/or other information that must be obtained, reviewed and analyzed; and
- The risk of significant complications, morbidity and/or mortality, as well as comorbidities associated with the patient’s presenting problem(s), the diagnostic procedure(s), and/or the possible management options.
The levels of the MDM are straightforward, low complexity, moderate complexity and high complexity. What makes it difficult for providers is that not much guidance has been provided as to how to identify the different elements or what makes up the difference between each level. Additionally, another thing that makes it difficult to determine is that to arrive at a particular level, providers and coders have to consider four categories, and within the table there are four corresponding types. To qualify for a level of MDM, the highest two of three elements must be met. In other words, one element does not equal your level of MDM. Often, the code selection is based solely on the risk of complications; however, keep in mind the other two elements play a role in determining the level of MDM. The level of MDM is determined by the table below:
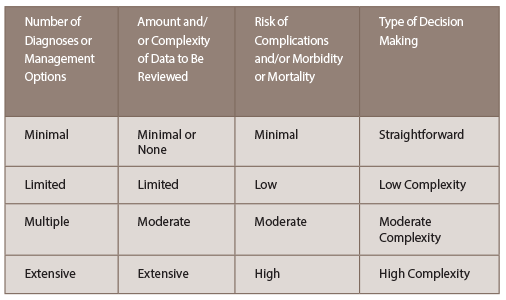
Number of Diagnoses or Management Options
This element is based on the number and types of problems, and the complexity of establishing a diagnosis, along with the management option that the rheumatologist will determine during the course of that visit. Because an established diagnosis that is not worsening would generally require fewer tests and data to review, it would be considered less complicated. A new problem, or a problem that is worsening, would require more work and, therefore, would be more complicated. Below are the documentation guidelines from the Evaluation and Management Services Guide:
