
Studio_G / shutterstock.com
The evaluation and management (E/M) code set in the American Medical Association’s Current Procedural Terminology (CPT) book lists descriptors, as well as typical times for patient visits. These times are averages of how long it takes a physician to complete all components of a visit at each level. Because the specific times identified in the CPT book are averages, they represent a range of times that may be higher or lower depending on actual clinical circumstances from visit to visit. It’s important to understand that time is only a contributing factor in determining which level of E/M to report.
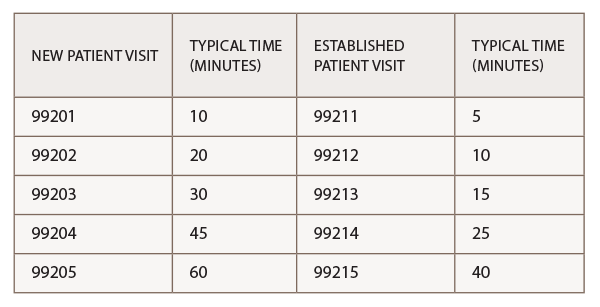
The key components of history, examination and medical decision making are usually used to determine an E/M level of service, if a provider ends up spending more than 50% of the total visit counseling and coordinating care, then time can be used as the key factor in determining the E/M level to bill for that service. Per the CPT, typical times for new and established office visits are:
When coding on the basis of time in the outpatient setting, providers can count only face-to-face time with the patient or family. This face-to-face time includes not only the time spent counseling, but also the time associated with any history, exam or medical decision making performed. Time spent reviewing records, talking with other providers and documenting the encounter without the patient or family present cannot be considered. It is not unusual for rheumatologists to spend significant time during an office visit reviewing new and/or existing problems, modifying medications, counseling and coordinating care. To determine whether to code for time as the key factor, the following questions must be answered:

