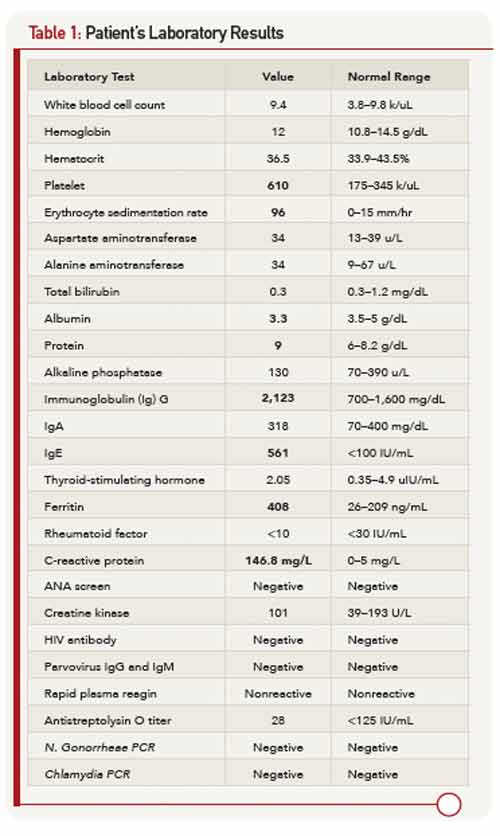
He was admitted to another hospital for further workup of his fever and polyarthritis. Laboratory workup revealed thrombocytosis and elevated inflammatory markers. Urinalysis demonstrated pyuria. All studies for infectious causes of his illness were negative. Other lab results are shown in Table 1. A chest X-ray was normal. Imaging of the hips and sacroiliac joints was normal. He was referred to the rheumatology clinic for further evaluation.
Our First Encounter
At age 10, the patient had developed a similar episode of painful arthritis, weight loss, and fevers up to 104º F. He was hospitalized for three weeks in Cape Verde, and was transferred to Portugal for further management. At that time, he was diagnosed with rheumatoid arthritis (RA), and treated with naproxen. Within six months, his symptoms completely resolved and he remained free of symptoms until his current presentation.
His past medical history included asthma. He was not taking any medications and had no allergies. His family was of Cape Verdian origin. A maternal cousin was diagnosed with arthritis during adolescence and was receiving monthly injections for his condition. There was no family history of lupus, thyroid disease, inflammatory bowel disease, psoriasis, or other autoimmune conditions. He was attending the 10th grade. He denied any alcohol or drug use and was not sexually active.
On physical examination, he was a tall, thin male using a wheelchair to enter the exam room. His blood pressure was 100/55 mm Hg, pulse 107 beats per minute, and he was afebrile. His weight was 113 pounds (32nd percentile), height 69 inches (78th percentile), and BMI 16.7 (7th percentile). His musculoskeletal exam was remarkable for left elbow arthritis, with full extension lacking by 10 degrees. His right elbow range of motion was normal. He had tenderness and swelling along the flexor tendon of the third digit of his right hand. There was slight sacroiliac joint tenderness bilaterally. The hip showed mildly decreased range of motion. The right knee had a small effusion and was tender at the insertion of the patellar tendon. His left knee was normal, and both knees had full range of motion. His ankles were warm, markedly swollen, and tender without overlying erythema. The Achilles tendons were swollen and tender bilaterally (see Figure 1). Both feet were swollen and tender, and he had dactylitis of the great toes. Gait could not be assessed because of pain. The nails were normal without pits, and there were no rashes. The rest of his exam was unremarkable.