Conservative follow-up treatment and rehabilitation did not improve the pain. Repeat MRI revealed an intact MCL autograft. An intra-articular corticosteroid injection was ineffective. He was released from the organization and presented to our ultrasound clinic seeking relief for his pain and hoping to resume his pitching career.
Exam
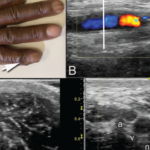
The examination revealed a well-healed incision over the left medial elbow. The medial epicondyle was nontender. No effusion was present, and his range of motion was normal. With elbow flexion, there was a suggestion of subluxation of the ulnar nerve outside the ulnar sulcus. On elbow extension, the ulnar nerve retracted back into the ulnar sulcus. No palpable snapping was noted on elbow flexion. A dynamic valgus stress test was negative. Left upper extremity muscle strength and sensation were intact.
Ultrasonography revealed the palmaris longus graft, which stretched from the medial condyle to the sublime tubercle of the ulna, was intact both statically and dynamically. No tears were noted. The ulnar nerve was 9 mm² in cross-sectional area, a normal value.
In elbow extension, ultrasonography revealed the ulnar nerve to be resting normally in the ulnar groove and without evidence of compression in the true cubital tunnel under Osborne’s ligament.
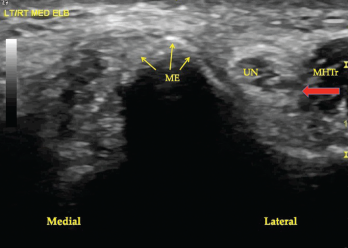
Figure 1. A transverse view of the ulnar groove in full elbow extension. The red arrow indicates the advancing edge of the MHTr.