Moving Toward Prevention
Along with providing better targeted therapeutics, underlying this research is the primary aim of preventing RA. “The field is moving toward prevention,” said Dr. Holers, adding that in the future rheumatologists may be able to detect patients at risk of RA or with the very earliest warning signs of disease by, for example, sputum testing that may reveal early pathophysiologic changes as described above.
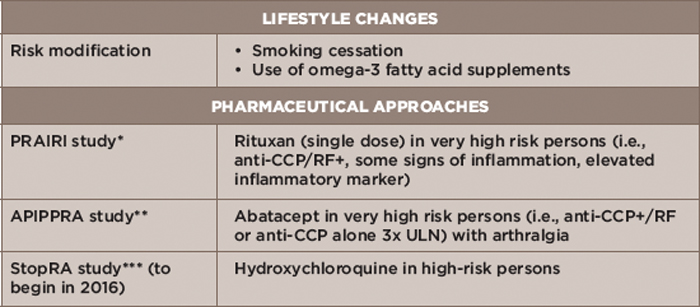
Table 3: Prevention Strategies
Key: CCP, cyclic citrullinated peptide; RF, rheumatoid factor; ULN, upper limit of normal
Notes: *Prevention of Clinically Manifest Rheumatoid Arthritis by B Cell Directed Therapy in the Earliest Phase of the Disease
**Arthritis Prevention in the Pre-Clinical Phase of RA with Abatacept
***Strategy to Prevent the Onset of Clinically Apparent Rheumatoid Arthritis
To that end, a number of RA prevention approaches are under investigation (see Table 3).