In general, typical first-line treatment for cutaneous lupus includes sunscreen and strict protection from UV exposure, topical and systemic steroids, topical calcineurin inhibitors and anti-malarial drugs. Second-line treatment includes methotrexate, mycophenolate, dapsone, belimumab, and, in recalcitrant patients, thalidomide or lenalidomide. Third-line treatments vary widely and are based largely on case series and anecdotal evidence, Dr. Merola said.
Dermatomyositis
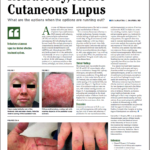
The classic clinical skin findings of this disorder, including the heliotrope and linear extensor erythema, are readily recognized by the rheumatologist. But, in darker-skinned patients, clinicians should look for areas of hyperpigmentation in the same locations one might have expected to find violaceous erythema. Some patients may present with eyelid edema with a heliotrope that is barely noticeable.
Dr. Merola
Novel antibodies have been found to help define clinical phenotypic subsets of dermatomyositis, including anti-MDA5, characterized by ulcerations on the hands and interstitial lung disease; and anti-TIF1-gamma, characterized by increased malignancy risk, widespread cutaneous disease, red and white patches, psoriasiform lesions and poikiloderma—areas of hypo- and hyper-pigmentation, telangiectasia and atrophy, Dr. Merola said.
Hydroxychloroquine for dermatomyositis is modestly effective for skin disease and photosensitivity in about 40% of patients, but with cutaneous drug hypersensitivity reactions occurring in up to a third of these patients, Dr. Merola said. More novel options include anti-interferon therapy and JAK inhibitors.2
TNF-Induced Psoriasiform Dermatitis
This disorder involves psoriatic lesions that arise due to treatment with anti-TNF drugs for other conditions, including rheumatic diseases and inflammatory bowel disease. The lesions typically appear within 10 to 30 months after the patient starts on the anti-TNF, but onset has been found to take as long as 105 months, Dr. Merola said. One study found that 72% of patients had no personal or family history of psoriasis.3
Infliximab, etanercept, adalimumab and certolizumab—essentially all of the anti-TNFs—have been found to be associated with the disorder.
In mild cases, a treat-through with continued use of the same anti-TNF drug generally works—with the use of such therapies as topical steroids, UV therapy and methotrexate for symptoms, Dr. Merola said.