Gts/shutterstock.com
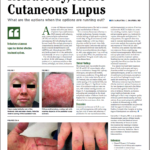
SAN FRANCISCO—A 40-year-old woman shows up in the clinic with scarring alopecia, with an area of hyperpigmentation on the rim of her scalp, extending from just behind the temple to behind her ears.
An examination with a dermatoscope shows hyperkeratotic follicular plugging.
Cutaneous lupus (CLE) grouping schemes can be somewhat confusing, with CLE broadly grouped into types with specific lesions and non-specific lesions—what is known as the Modified Gilliam Grouping Schema. The so-called lupus specific lesion group is then sub-grouped into acute cutaneous LE, subacute LE and chronic cutaneous LE, which includes DLE.
There are limited data to answer the question of SLE risk, said Dr. Merola, who is dual-certified in dermatology and rheumatology. But cross-sectional prevalence data are available, he said. In DLE, localized lesions—those above the neck—are associated with SLE in around 5% of patients, while generalized lesions, about 20%. It seems that among those patients with DLE who are going to progress to SLE, the majority do so within five years of DLE diagnosis. Unpublished data at Dr. Merola’s center suggest this might happen much sooner than five years out, he said.
Subacute cutaneous LE (SCLE) is associated with SLE about 50% of the time; acute CLE, including malar eruption, about 90%. Lupus panniculitis is associated with SLE about 10% of the time, while tumid CLE, a rare variant of the chronic cutaneous form, essentially never does, Dr. Merola said.
Despite earlier reports, it appears that SLE patients with DLE are at a lower risk of arthritis and serositis than SLE patients without DLE, but have about the same risk of nephritis and end-stage renal disease.1
Subacute Cutaneous Lupus Erythematosus (SCLE)
There is an ever-increasing number of medications associated with drug-induced SCLE. A frequent question that arises when patients present with SCLE is whether it is idiopathic or drug induced. Dr. Merola presented an example of a patient who was started on adalimumab for seropositive, erosive rheumatoid arthritis two months earlier, and had a biopsy that was “consistent with connective tissue disease including cutaneous lupus.” She was also positive for anti-SSA/Ro antibodies.
Drug-induced SCLE tends to have more widespread distribution, and those anti-SSA/Ro antibodies will disappear in more than three-quarters of patients after it is resolved. Tissue eosinophilia is not a distinguishing factor on histopathology, Dr. Merola said.
Cardiovascular medications, including hydrochlorothiazide, calcium channel blockers, ACE inhibitors, beta blockers and statins are all associated with SCLE. So are tumor necrosis factor (TNF) alpha inhibitors, proton-pump inhibitors and many medications commonly used for cancer.
In general, typical first-line treatment for cutaneous lupus includes sunscreen and strict protection from UV exposure, topical and systemic steroids, topical calcineurin inhibitors and anti-malarial drugs. Second-line treatment includes methotrexate, mycophenolate, dapsone, belimumab, and, in recalcitrant patients, thalidomide or lenalidomide. Third-line treatments vary widely and are based largely on case series and anecdotal evidence, Dr. Merola said.
Dermatomyositis
The classic clinical skin findings of this disorder, including the heliotrope and linear extensor erythema, are readily recognized by the rheumatologist. But, in darker-skinned patients, clinicians should look for areas of hyperpigmentation in the same locations one might have expected to find violaceous erythema. Some patients may present with eyelid edema with a heliotrope that is barely noticeable.
Dr. Merola
Novel antibodies have been found to help define clinical phenotypic subsets of dermatomyositis, including anti-MDA5, characterized by ulcerations on the hands and interstitial lung disease; and anti-TIF1-gamma, characterized by increased malignancy risk, widespread cutaneous disease, red and white patches, psoriasiform lesions and poikiloderma—areas of hypo- and hyper-pigmentation, telangiectasia and atrophy, Dr. Merola said.
Hydroxychloroquine for dermatomyositis is modestly effective for skin disease and photosensitivity in about 40% of patients, but with cutaneous drug hypersensitivity reactions occurring in up to a third of these patients, Dr. Merola said. More novel options include anti-interferon therapy and JAK inhibitors.2
TNF-Induced Psoriasiform Dermatitis
This disorder involves psoriatic lesions that arise due to treatment with anti-TNF drugs for other conditions, including rheumatic diseases and inflammatory bowel disease. The lesions typically appear within 10 to 30 months after the patient starts on the anti-TNF, but onset has been found to take as long as 105 months, Dr. Merola said. One study found that 72% of patients had no personal or family history of psoriasis.3
Infliximab, etanercept, adalimumab and certolizumab—essentially all of the anti-TNFs—have been found to be associated with the disorder.
In mild cases, a treat-through with continued use of the same anti-TNF drug generally works—with the use of such therapies as topical steroids, UV therapy and methotrexate for symptoms, Dr. Merola said.
With moderate to severe disease, switching to a different anti-TNF, along with treating the symptoms, is recommended.
“[In] switching to another anti-TNF, particularly moving from infliximab to another,” Dr. Merola said, “we’ve had reasonable success, much higher than what was reported in at least some case series.”
For moderate to severe disease that is recalcitrant or worsening, it’s probably best to consider switching to another mechanism of action, based on the patient’s underlying disease state, he said. Patients with IBD, for instance, may be transitioned to ustekinumab, and rheumatoid arthritis patients to abatacept.4 Clinically, he said, many patients present with a variant of plaque disease that has overlapping features with eczema—spongiotic psoriasiform dermatitis on histopathology—as well as pustular variants, including palmo-plantar pustular psoriasis.
Thomas R. Collins is a medical writer based in Florida.
References
- Merola JF, Prystowsky SD, Iversen C, et al. Association of discoid lupus erythematosus with other clinical manifestations among patients with systemic lupus erythematosus. J Am Acad Dermatol. 2013 Jul;69(1):19–24.
- Hornung T, Janzen V, Heidgen FJ, et al. Remission of recalcitrant dermatomyositis treated with ruxolitinib. N Engl J Med. 2014 Dec 25;371(26):2537–2538.
- Afzali A, Wheat CL, Hu JK, et al. The association of psoriasiform rash with anti-tumor necrosis factor (anti-TNF) therapy in inflammatory bowel disease: A single academic center case series. J Crohns Colitis. 2014 Jun;8(6):480–488.
- Sandborn WJ, Gasink C, Gao LL, et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N Engl J Med. 2012 Oct 18;367(16):1519–1528.