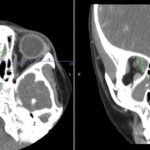
Figure 1: Destructive naso-orbital lesion. Note the soft-tissue mass extending into the orbit with destruction of the left median orbital wall.
Imaging of the orbit demonstrated destruction involving the left lateral nasal wall, floor of the orbit, middle turbinate, roof of the nasopharynx, and the sphenoid sinus with abnormal soft tissue density along the left medial orbital wall and orbital floor with extension through several skull base foramina (see Figure 1). A chest CT demonstrated a right-middle lobe cavitary lesion measuring 2 cm by 2 cm with a small satellite lesion (see Figure 2). An abdominal CT demonstrated a locally invasive process involving the prostate gland, bladder, and seminal vesicles, as well as a 2.7cm by 2.1 cm renal mass (see Figure 3).