click for large version
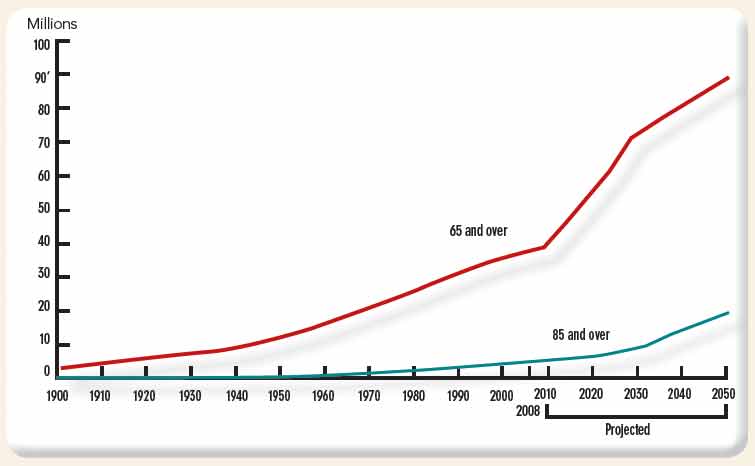
Population age 65 and over and age 85 and over, selected years 1900–2008 and projected 2010–2050
Note: Data for 2010–2050 are projections of the population. Reference population: These data refer to the resident population. Source: U.S. Census Bureau, Decimal Census, Population Estimates and Projections.
Note: Data for 2010–2050 are projections of the population. Reference population: These data refer to the resident population. Source: U.S. Census Bureau, Decimal Census, Population Estimates and Projections.
Balanced Treatment
Any treatment in the geriatric population should receive additional consideration to avoid causing further bodily harm. “In this population, where these individuals may be more frail, perhaps more socially isolated, with more multimorbidity and polypharmacy, we have to be especially careful and cognizant of the potential benefits and harms of our treatment,” Dr. Makris says.


