Baricitinib is a preferential JAK1 and JAK2 inhibitor that has completed Phase 2 clinical trials, the results of which were published in 2015.
Baricitinib is a preferential JAK1 and JAK2 inhibitor that has completed Phase 2 clinical trials, the results of which were published in 2015.
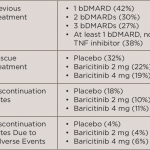
In a recent Phase 3 study, baricitnib was used to treat patients with rheumatoid arthritis (RA) who had an inadequate response to or unacceptable side effects from more than one tumor necrosis factor inhibitor or other biologic disease-modifying anti-rheumatic drug (DMARD).1 This study was the RA-BEACON trial, which was a randomized, 24-week, double-blind, placebo-controlled study in 24 countries and 178 centers.