click for large version
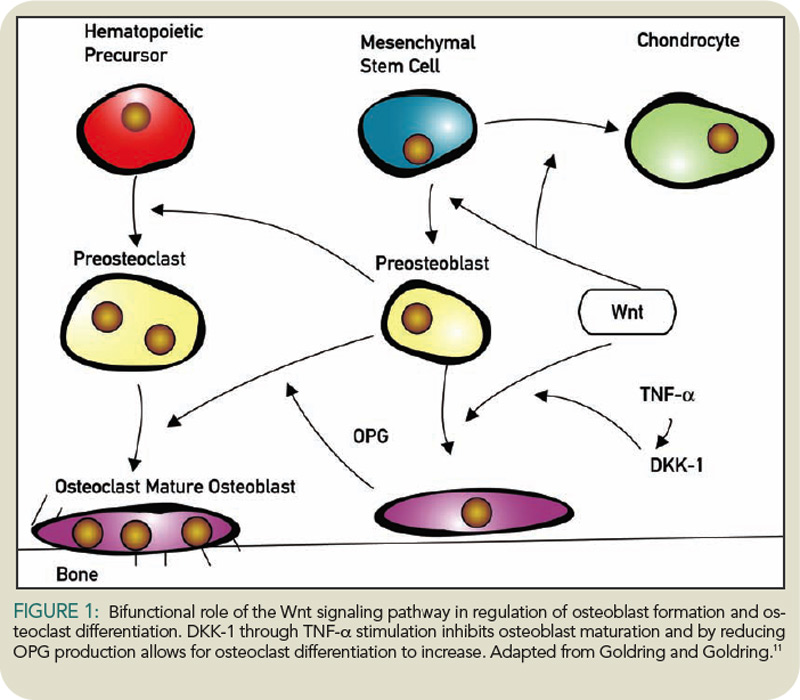
figure 1: Bifunctional role of the Wnt signaling pathway in regulation of osteoblast formation and osteoclast differentiation. DKK-1 through TNF-a stimulation inhibits osteoblast maturation and by reducing OPG production allows for osteoclast differentiation to increase. Adapted from Goldring and Goldring.11
Therapies: Anabolic Agents
Teriparatide (PTH), which is approved for the treatment of osteoporosis, differs from the anti-resorptive agents in its actions. PTH is an anabolic agent that stimulates osteoblasts to form new bone while simultaneously increasing osteoclastic bone resorption through increasing receptor activator for nuclear factor k B ligand factor (RANKL) production. While bone turnover is increased with PTH, overall bone mass and bone strength increase with this agent, reducing fracture risk. While PTH is approved for the treatment of osteoporosis, it is generally not used as a first-line agent because of cost and the need for injections.

