When interviewing a patient with Behçet’s disease & new-onset headache, reports of morning headache, a positional component, worsening with Valsalva & refractoriness to therapy should prompt a cerebral venous sinus thrombi workup.
Neuro-Behçet Disease
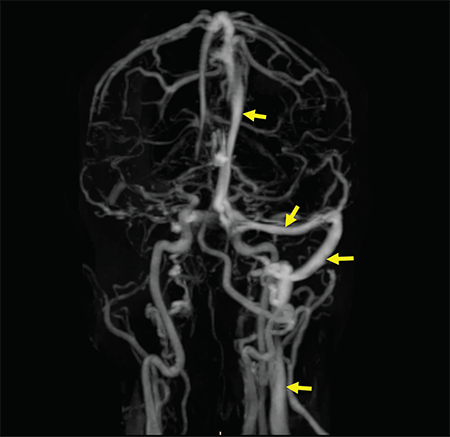
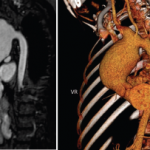
Figure 2: A contrast-enhanced MRV shows a filling defect in the right internal jugular vein, right sigmoid sinus, right transverse sinus and superior sagittal sinus. Normal enhancement of the respective structures is visualized on the left side (arrow).
As a multisystem inflammatory disease, Behçet’s disease can affect any organ or system in the body, including the nervous system. Neurological manifestations in Behçet’s disease are generally divided into parenchymal (intra-axial) and non-parenchymal (extra-axial). A diagnosis of neuro-Behçet disease is considered in patients who fulfill Behçet’s disease diagnostic criteria, do not have an alternative explanation for neurological symptoms and have supportive objective evidence of abnormal cerebrospinal fluid (CSF) analysis and/or abnormal MRI imaging.5