Investigations
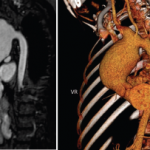
In a patient with Behçet’s disease who presents with headache, if CVST is suspected, neuroimaging evaluation with MRI and MRV should be promptly performed to assess for venous sinus and deep vein occlusion, and to rule out other causes of headache, such as mass or hemorrhage.
Lumbar puncture should also be considered to aid with excluding other causes of severe headache, such as infection. Cerebrospinal fluid (CSF) analysis can be normal, but if abnormal, the most notable findings are elevated opening pressure and lymphocytic predominant elevated cell count. 5,6
Once CVST is confirmed, screening for vascular disease at an extracranial site is recommended by current guidelines.10.11 Many patients with this complication present to tertiary medical centers with a known diagnosis of CVST and on anticoagulation, so it’s not always feasible to perform lumbar puncture.
Although Behçet’s disease is a predisposing factor for development of CVST, other pro-thrombotic factors can often be found in patients with Behçet’s disease. A study of 64 patients with Behçet’s disease and CVST found at least one other associated pro-
thrombotic factor in 31% of the cases, including methylenetetrahydrofolate reductase gene mutation, hyperhomocysteinemia, protein C deficiency and factor V Leiden mutation. Other environmental pro-thrombotic risk factors, such as smoking status and use of estrogen-containing contraceptive methods, were also reported in 34–36% of cases of CVST in the same study.12
Treatment
The general therapeutic approach in treating Behçet’s disease-associated CVST is to optimize immunosuppression, given that the underlying mechanism is inflammation of the vessel wall.10 This is commonly achieved with high-dose glucocorticoids, pulse dose or 1 mg/kg, followed by a slow taper over several months. Other immunosuppressive therapies used concomitantly as steroid-sparing medications include cyclophosphamide, azathioprine and TNF inhibitors for severe or refractory cases.10,12,13
The EULAR guidelines for management of Behçet’s disease recommend against the use of cyclosporin-A, due to available data from observational studies that suggest cyclosporin-A increases the risk of nervous system involvement in patients with Behçet’s disease due to its neurotoxic effects.10,11 Immunosuppressive therapy has been shown to significantly reduce the risk of CVST recurrence.13,14
Due to a lack of evidence from clinical trials and presumed increased risk of bleeding associated with anticoagulation, no clear consensus exists on the use and duration of anticoagulation for thrombosis in Behçet’s disease.10,15 That said, most experts in the U.S. would likely recommend anticoagulation until the thrombosis resolves, as long as there are no contraindications.
In a retrospective study of 21 Behçet’s disease patients with CVST, except for one patient with hemoptysis and subarachnoid hemorrhage, all received long-term anticoagulation without any adverse effects.13 Similarly, in a prospective, placebo-controlled trial of 64 patients with CVST, over 90% received long-term anticoagulation without severe hemorrhagic complications, and the outcomes of those treated with anticoagulation were not worse than those treated with immunosuppressive therapy.12