Discussion
Diagnosing SAIDs can be an arduous process because the conditions often share identical clinical phenotypes and their presentations often mimic infectious, malignant, allergic and autoimmune disorders, particularly early in the course of disease. A broad differential diagnosis is invariably required and should also include the newly discovered group of autoinflammatory disorders.5,6
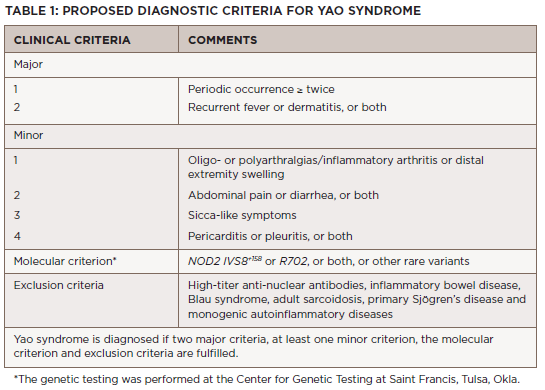
The diagnosis of Yao syndrome requires the presence of clinical criteria, consisting of typical symptoms; molecular criteria, consisting of NOD2 variants; and the proper exclusion of similar diseases, such as inflammatory bowel syndrome, sarcoidosis, Sjögren’s disease, Blau syndrome and other monogenic autoinflammatory syndromes.3,7 The NOD2 variant IVS8+158 is detected in almost all patients with Yao syndrome, with concurrent R702W in up to 30%.3,7
Click to enlarge.
Recently, our growing understanding of the disease has identified even newer genetic variants and other unique manifestations, such as eyelid swelling.8 Table 1 shows the proposed diagnostic criteria for Yao syndrome.9
Differentiating Yao syndrome from other hereditary periodic fever syndromes is an essential part of the diagnostic evaluation.4 Of the autoinflammatory disorders, familial Mediterranean fever (FMF) appears to have the closest phenotypic overlap with Yao syndrome despite having its own distinct genetic mutation in the MEFV gene.

