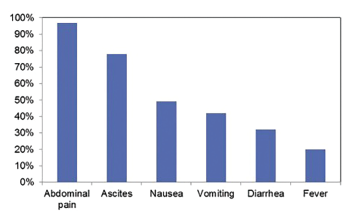
Figure 3: Incidence of Symptoms at Presentation with Lupus Enteritis3
Since 2015 she has had intermittent flares, attributed to SLE, with rashes on her hands and joint pain, predominantly in her hands. Flares tended to be cyclic and related to her menses. She self-managed her symptoms with stress reduction and homeopathic modalities. She had no recent hospitalizations or steroid tapers. She did not think her current symptoms were typical of an SLE flare, and she was taking no medications at the time of presentation.
Review of Systems
The patient had chronic hair loss, difficulty taking a deep breath due to abdominal pain, esophageal reflux, abdominal pain, nausea, vomiting, diarrhea, anorexia, rash on her hands and an oral ulcer. She denied fevers, chills, weight loss, joint pain or swelling, chest pain, headaches, vision changes, dyspnea, dysuria, hematuria, weakness, leg swelling, seizures, blood clots, miscarriages, recent travel, sick contacts, a history of inflammatory bowel disease or Raynaud’s phenomenon.

