Discussion
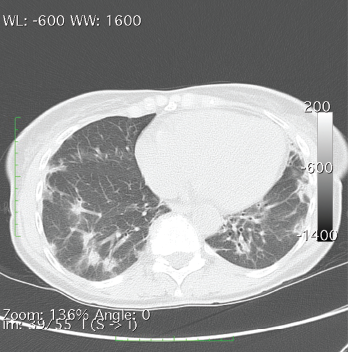
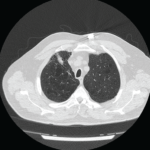
A CT of the chest without contrast showed multiple nodular and coalescing opacities involving the bilateral lungs diffusely, with more extensive involvement of the bibasilar regions.
Dermatomyositis encompasses a host of musculoskeletal and cutaneous symptoms, the latter of which are often heterogeneous in presentation. It is thought that differing serological responses, as reflected via various antibody markers, may represent differing immune responses, even unique phenotypes, with associated keratinocyte damage, which may explain the heterogeneity of presentation.4,5
MDA5, a receptor that binds with RNA and triggers a type I interferon response in infectious and inflammatory processes, was discovered in 2002 and has since become a point of interest in the study of autoimmune processes.6 Among patients with DM, certain features are strongly associated with anti-MDA5, including the absence of myositis and the presence of palmar papules, periungual, digital and elbow cutaneous ulcers, and rapidly progressive ILD, suggesting a unique phenotype that may pose its own treatment challenge.5