Click to enlarge.
Review of systems: He reported migratory polyarthritis, recent ocular pain and redness, and chronic low back pain and stiffness. The patient denied any skin rash, such as psoriasis; constitutional symptoms, including fever, chills, weight loss and night sweats; dactylitis; gastrointestinal or genitourinary symptoms; nasal discharge, crusting or bleeding; nasal or auricular chondritis; sinus or respiratory symptoms, such as cough, hemoptysis or shortness of breath; sore throat; numbness or tingling sensation in his extremities; recent infection, including sexually transmitted disease; or tick bite preceding his symptoms.
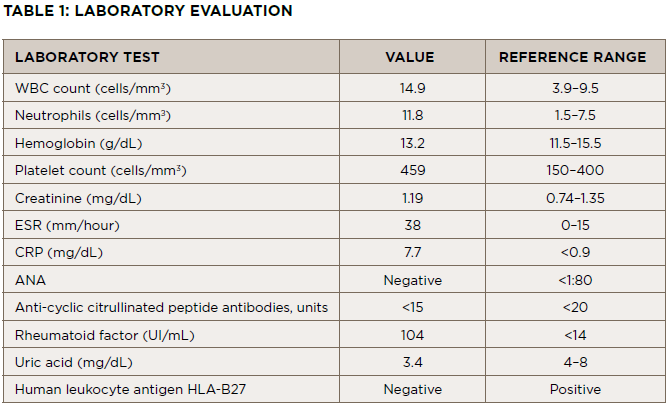
Physical examination & laboratory evaluation: Upon evaluation, the patient was afebrile (98ºF), had a blood pressure of 123/83 mmHg, a heart rate of 90 beats per minute and a normal respiratory rate.

