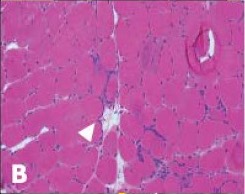
FIGURE B: Endomysial infiltrates (arrowheads) and rimmed vacuoles on biopsy.
Lack of consistent longitudinal specialty care hindered patient-centered communication and care. As Mr. F’s physical decline made regular travel to our specialty center impractical, his only contact with the medical system occurred when he was hospitalized. The providers he encountered were unfamiliar with the management and progression of IBM, preventing informed communication about care and prognosis. Although he was frequently in contact with the medical system, he had no conversations with clinicians about his prognosis, advance care planning or the implications of his progressive disease.
During one hospitalization for aspiration pneumonia, he underwent swallow studies that demonstrated significant dysmotility and was told he was no longer allowed to eat or drink by mouth. A percutaneous endoscopic gastrostomy (PEG) tube was placed with minimal conversation or guidance. He was told that he essentially had no choice in the decision because if he continued to eat and drink by mouth, he would die. After diligently not eating by mouth for a year, he felt overwhelmed by the emotional ramifications and the impact on his quality of life. With the support of his wife, he chose to begin eating by mouth once again, recognizing the risk of developing aspiration pneumonias. While his wife was supportive, every time he was hospitalized for aspiration he was criticized by his healthcare team for his decision to attempt oral feeding.
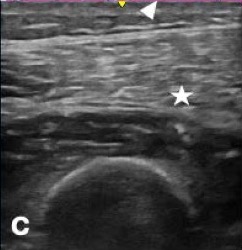
FIGURE C: Muscle ultrasound with increased echo intensity of vastus lateralis.
Goals-of-care discussions took place only in the days before his death. During a hospitalization for respiratory failure, for which Mr. F was admitted to the intensive care unit (ICU), Mrs. F ultimately asked for palliative care to be involved. The ICU team agreed, but Mr. F’s primary care doctor felt this decision was akin to giving up. Eventually, Mr. F passed away in the ICU due to respiratory failure secondary to IBM.
The unpredictability of Mr. F’s illness, combined with the lack of medical guidance throughout the process, led to significant distress for Mr. and Mrs. F. “You know what I think the problem was?” Mrs. F says, “I don’t think I knew when it was the end of life. There was a constant [uncertainty]. … Is it going to be this year or month? There were so many times I thought he was going to pass but he didn’t.”


