Reflecting back, Mrs. F thinks earlier goals-of-care conversations would have been helpful. And as Mr. F continued to decline, there was no central person to guide them through the process.
Discussion
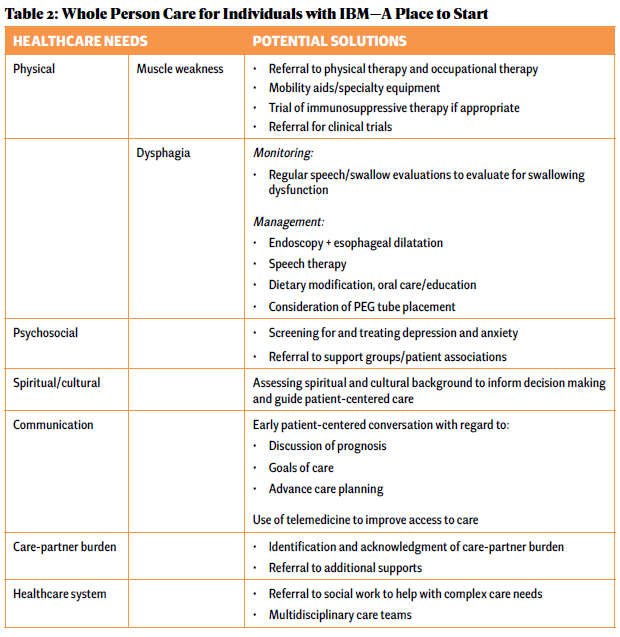
IBM is a serious and devastating illness without any known, effective cure. Excellent person-centered care of patients with IBM and their care partners must include palliative care—identification and management of total suffering, which includes physical, psychosocial, spiritual/existential and financial distress. Increasing access to palliative care requires educating rheumatologists about how to incorporate palliative care modalities into their management framework and identifying when referral to specialty palliative care is appropriate (see Table 2).
Click to enlarge.
Complex symptom management is part of holistic IBM care.
Like Mr. F, many individuals with IBM have limited contact with the healthcare system after diagnosis because of the perception that available medical care is futile given the incurable nature of the disease; however, addressing symptom burden may not only relieve suffering, but may also improve the patient’s ability to continue receiving IBM-directed therapies.
For example, regular evaluation for swallowing dysfunction can allow for earlier interventions with such procedures as esophageal dilations or speech therapy, and prompt early conversations regarding PEG placement.6,7 Management of dysphagia, such as dietary modification, oral care and education, can be beneficial in managing symptoms for individuals with IBM and progressive swallowing dysfunction.8


