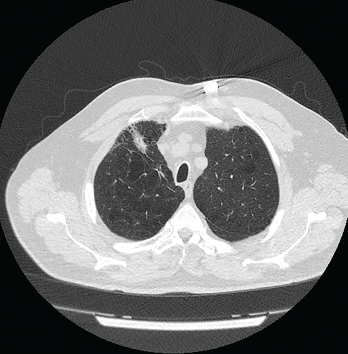
Figure 1: Computed Tomography VGstockstudio / shutterstock.com
Pulmonary nodules are common; most are benign, but the differential diagnosis is broad and includes life-threatening possibilities.1 Our patient is a former smoker who has a history of a complex autoimmune disease and multiple pulmonary nodules. This case was challenging, but clinical, radiographic and histologic clues helped lead to the correct diagnosis.
Case Presentation
The patient is a 74-year-old man with a past medical history remarkable for hypertension, hyperlipidemia, gastroesophageal reflux disease, emphysema, asbestos exposure and seropositive (rheumatoid factor and anti-cyclic citrullinated protein antibody) rheumatoid arthritis/scleroderma/systemic lupus erythematosus (SLE) overlap syndrome. He has a 100 pack-year smoking history, although he quit smoking 22 years ago.

