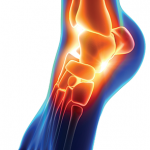
Figure 1: A lateral view of the right foot/ankle is shown with associated erythema and joint inflammation from the ankle to the forefoot. You can appreciate the associated swelling of the left medial ankle in the background, as well.
SARS-CoV-2, or COVID-19, is a complex disease entity that continues to evolve. Physicians, researchers and scientists alike have worked tirelessly to tackle this beast in its short existence; however, we are reminded daily that there is more to this virus than meets the eye. It is well known that COVID-19 can cause acute respiratory failure along with extra-pulmonary manifestations, including thromboembolic events and cardiac manifestations. Perhaps less commonly known, patients may also experience musculoskeletal manifestations.
Below, we discuss the case of a 21-year-old man who presented with inflammatory arthritis and tenosynovitis following a diagnosis of COVID-19.