Left: A transverse view of the posterolateral left (affected) knee at the level of the fibula.
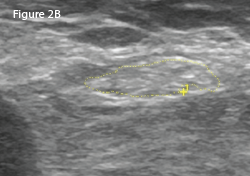
Right: The same view as 2A, with the common peroneal nerve outlined in yellow with a cross-sectional area of 21 mm2.
LEFT: A transverse view of the posterolateral right (unaffected) knee at the level of fibula.
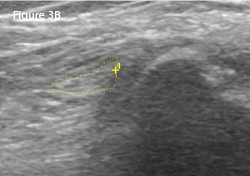
RIGHT: The same view as 3A, with the common peroneal nerve outlined in yellow with a cross-sectional area of 8 mm2.
Subsequent electrophysiologic studies (EPS) revealed the left superficial peroneal nerve sensory portion to be unresponsive, suggestive of peroneal nerve compression. Motor function of the nerve was intact.
It was concluded the mildly tender neuroma was not clinically significant in comparison with the ultrasonic findings of the left CPN, supported by the abnormal EPS.
CPN neuropathy has been described as a rare occurrence following total & unicompartmental knee arthroplasty.
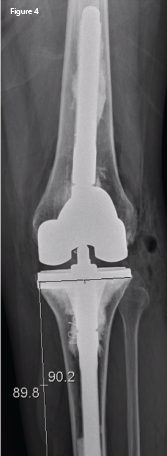
An anteroposterior X-ray of the left knee following revision arthroplasty. The lateral femoral and tibial overhang has been eliminated.
The patient agreed to a second TKA revision for progressive varus deformity. A smaller prosthesis was used, with the intention of decompressing the common peroneal nerve and eliminating the varus deformity. Figure 4) demonstrates the TKA revision with correction of both the tibial and femoral lateral overhang.
Seven months post-operative, the patient reported her pain—and ADLs—to be markedly improved.
Discussion
Etiology of Peroneal Neuropathy at the Knee
The sciatic nerve arises from the lumbosacral ventral rami and divides into the common peroneal and tibial nerves just proximal to the popliteal fossa. The CPN, which receives contributions from L4–5 and S1–2, courses lateral to the biceps femoris tendon and fibula head, a location vulnerable to injury.
Common peroneal nerve palsy may occur with tibia and fibula fracture, knee dislocation, sports injuries, iatrogenic surgical trauma, compression from a ganglion cyst, osteochondroma, aneurysm and various mass lesions.1-8 Excessive weight loss may predispose a patient to CPN neuropathy as well.9-11 Although the precise incidence is unknown, CPN neuropathy has been described as a rare occurrence following total and unicompartmental knee arthroplasty.1,7,8,12 The mechanism of CPN neuropathy after TKA is unclear, but may be due to soft tissue compression or traction on the nerve.8
Clinical Presentation of Peroneal Neuropathy after TKA
Peroneal neuropathy after knee arthroplasty may manifest as weakness, persistent radiating pain, loss of sensation and paresthesias—all symptoms that interfere with rehabilitation and ADLs.1,7,8,12 Of interest is that CPN neuropathy after TKA may exhibit nonspecific symptoms, including localized pain and decreased range of motion, which may also hinder full functional recovery.1 This has been described as CPN dysfunction, but may still be definitively diagnosed by EPS.1
Traditional Evaluation of Suspected Peroneal Nerve Injury