An X-ray of his chest was unremarkable, but a computed tomography (CT) scan of the abdomen revealed diffuse mesenteric nodules in the peritoneum. An exploratory laparotomy revealed punched-out, noncaseating granulomas, with evidence of focal necrosis, concerning for sarcoidosis or Q fever (Coxiella burnetii infection).
A multi-disciplinary review received from other hospitals concluded the patient likely had either sarcoidosis or Q fever. Kveim testing was negative. The patient was not started on any treatment and was lost to follow-up.
In the following years, the patient continued to experience intermittent episodes of abdominal pain. He did not seek medical care during this time, in part due to frustration with the inability of physicians to offer him a firm diagnosis.
In 2022, he presented to the emergency department with intractable, diffuse abdominal pain, fevers to 102ºF and diaphoresis. He also reported chronic diarrhea and intermittent blurry vision.
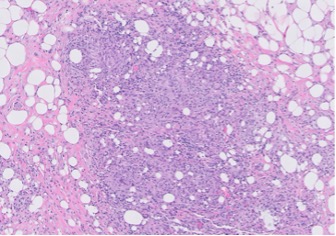
FIGURE 1A: Loose granuloma/swirling histiocytes and admixed acute inflammation can be seen in mesenteric fat. (Click to enlarge.)
A rheumatologist ordered laboratory tests for anti-nuclear antibody (ANA), rheumatoid factor, anti-CCP antibody, SSA/SSB, anti-neutrophil cytoplasmic antibodies (ANCA), myeloperoxidase (MPO) and proteinase (PR3), all of which were normal. Evaluation for HIV, tuberculosis, Strongyloides and Q fever was negative.


