Compared with the CT scan of the patient’s abdomen from 2007, the current CT scan revealed ill-defined infiltration of the omentum and mesentery. Diagnostic laparoscopy, lysis of adhesions, omental and small bowel biopsy were performed.
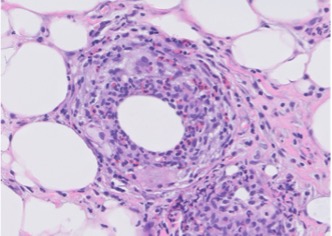
FIGURE 1B: Histiocytes associated with eosinophils are present. (Click to enlarge.)
Pathology revealed donut-shaped, non-necrotizing epithelioid granulomas with punched-out central spaces and rare, silver birefringent crystals, atypical for sarcoidosis and more suggestive of a foreign body reaction (see Figures 1A & 1B). The patient was also incidentally found to have elevated liver enzymes. Hepatitis serologies and anti-smooth muscle antibodies were negative. Because his liver enzymes continued to rise, a liver biopsy was performed, and the results were consistent with a nonspecific reactive hepatitis possibly due to a drug reaction unrelated to his granulomatous disease.


