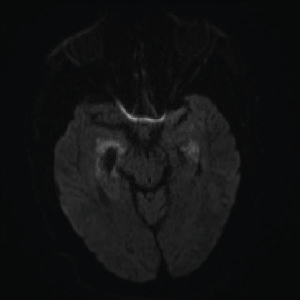
Image 1A: DWI: Diffusion seen bilaterally, particularly in the mesial temporal lobe.
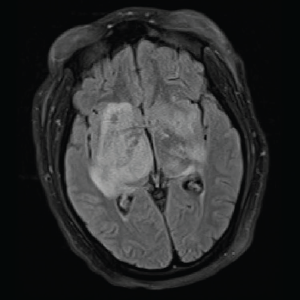
Image 1B: T2/FLAIR: Hyperintensities of the bilateral mesial temporal lobes extending into the right basal ganglia.
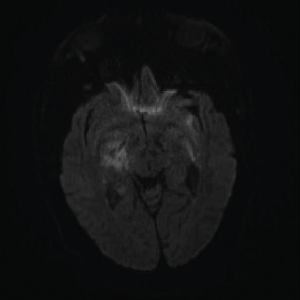
Image 2: DWI: Extensive abnormal signal with patchy areas of restricted diffusion, particularly in the right basal ganglia and bilateral mesial temporal lobes.
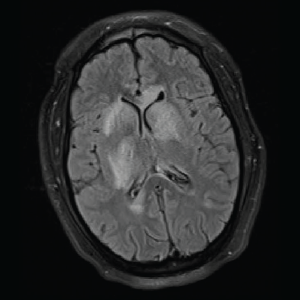
Image 3: T2/FLAIR: Hyperintensities of the caudate nucleus with mild mass effect.
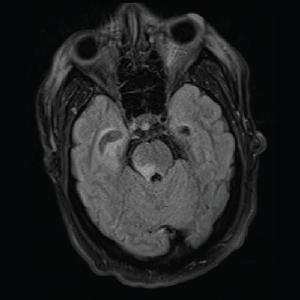
Image 4: T2/FLAIR: Abnormal T2/FLAIR signal of the right midbrain and pons.
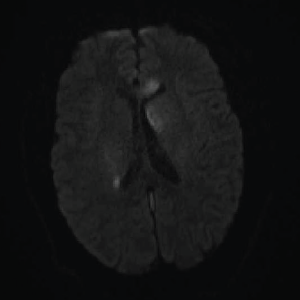
Image 5: DWI: Extensive areas of restricted diffusion extending to the periventricular white matter along the lateral ventricles.
By now a multidisciplinary team, which included infectious disease, pulmonology/critical care, rheumatology, neurology and hospitalist service, was working together to evaluate the case. They sent laboratory workup for infectious and autoimmune etiology. Complete blood count (CBC) showed normocytic anemia, lymphopenia, normal leukocytes and normal platelet counts. Inflammatory markers were elevated (ESR >130 mm/hr and C-reactive protein = 15.6 mg/dL—see Tables 1 and 2, below and opposite). A drug screen was positive for the oxycodone the patient had received a prescription for during his previous admission. Blood, urine and CSF cultures were all negative for bacterial, viral and fungal etiology (see Table 1).

