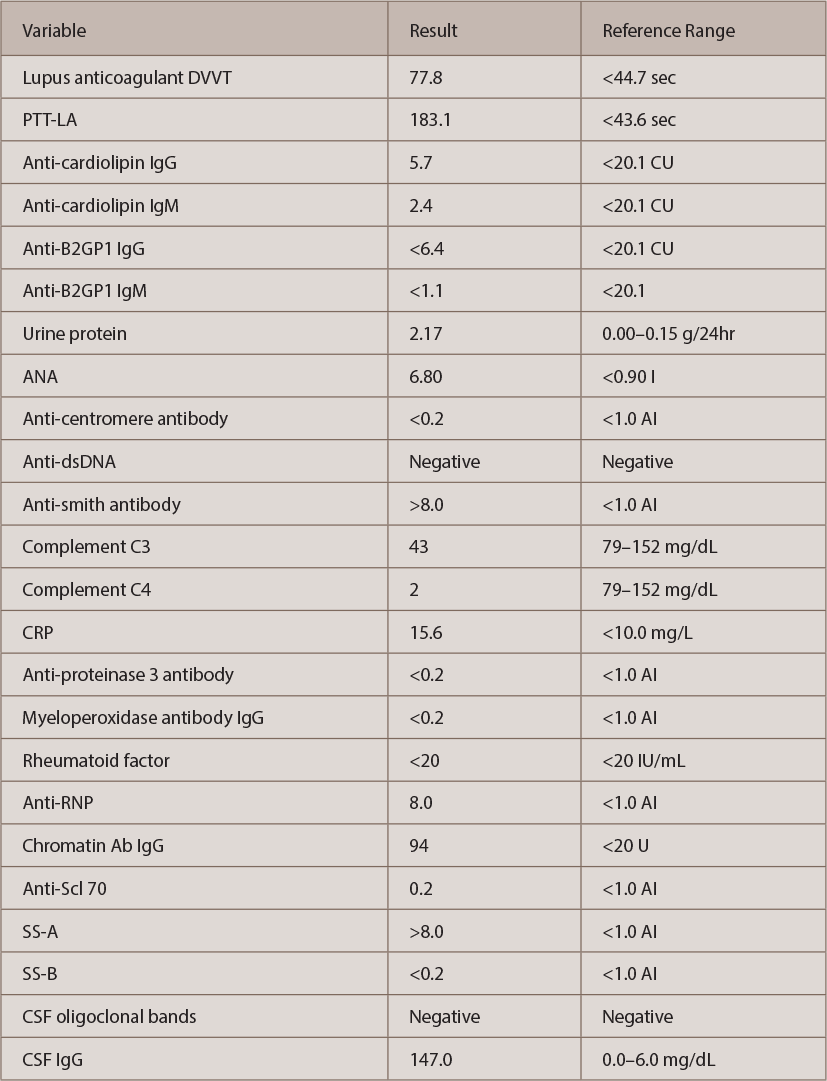
Autoimmune workup revealed positive antinuclear antibody (ANA) (titer 1:640, speckled pattern). ANA subset serology identified positive SS-A, ribonucleoprotein and anti-Smith antibodies. Interestingly, double-stranded DNA (ds-DNA) and SS-B were negative (see Table 2, opposite). An antiphospholipid antibody panel was positive for elevated lupus anticoagulant, but it might have been falsely positive because the patient was already on anticoagulation with a direct thrombin inhibitor started a few weeks before this admission for DVT.
(click for larger image)
Table 2: The Patient’s Autoimmune Evaluation
Urinalysis was positive for nephritic range proteinuria (protein in urine was 2.17 g/24 hr); hypoalbuminemia was noted (2.0 g/L) as well. Urine and serum electrophoresis were also completed, and were negative for monoclonal protein. MRI of the cervical spine and a CT angiogram of the patient’s head and neck were also completed, and showed no signs of vasculitis.

