Diagnoses & management options: Document the number of problems addressed during the visit that are relevant to the presenting problem. If there is a new problem, verify that this is clearly stated in the history of present illness, review of systems or examination. Showing how the patient condition is being handled is at the heart of disease management. The history and examination are not always enough to reach a diagnosis, so it is important to document what other work was done to arrive at a definitive diagnosis.
Data: The guidelines state there may be a need to look at “the amount and complexity of data to be reviewed.” This refers to information from sources other than the history and physical, lab tests, imaging, other diagnostic services, old records and history from sources other than the patient. This shows an increase in the complexity and volume of data you will need to review or order to help with the quality of care. Key factors to document for the data component include:
- the nature of any diagnostic service you order, plan, schedule or perform at the time of the encounter;
- any review of diagnostic test results that you perform;
- any decision to review old records or obtain history from sources other than the patient;
- relevant findings from any review of old records or from any additional history you obtain that will aid in verifying a diagnosis or in any treatment options;
- the results of any discussion you have with the physician who carried out or interpreted a diagnostic test or service; and
- “direct visualization and independent interpretation of an image, tracing or specimen” that has been or will be interpreted by another physician.
Such independent checking is not expected to be a regular thing, but rather something that rarely happens.
Risk: The guidelines consider risk to the patient in determining the level of medical decision making—risk of significant complications, morbidity and mortality—and they recognize three gauges of this risk: the presenting problems, any diagnostic procedures you choose and any management options you choose. Key documentation principles to follow for this component are outlined in Table 1.
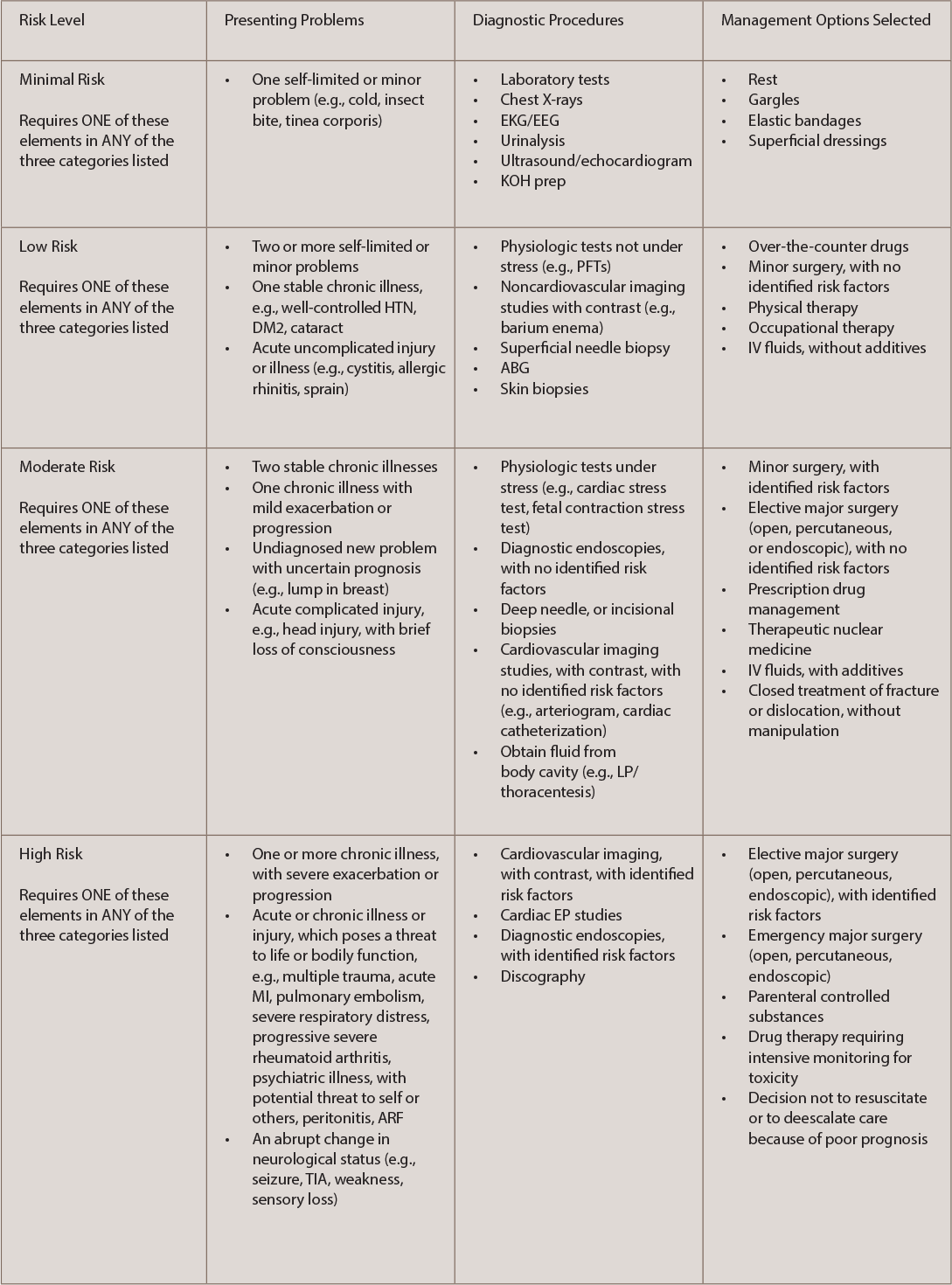
(click for larger image) TABLE 1: Key Risk Documentation Principles
The comprehensive process in medical decision making is an area that reflects evaluating, testing and treatment, and providers should take precaution to monitor practice improvement to avoid unnecessary audits and/or coding adjustments.
Keep in mind that Medicare and private payers incorporate medical necessity as a criterion for payment in addition to the individual requirements of the CPT codes. Thus, when CMS states that the medical necessity requirement must be met “in addition to the individual requirements of a CPT code,” this means, even if a service meets the technical requirements of a CPT code level (including medical decision making), that level may be higher than the medical necessity of the service, which may make it unpayable by Medicare at that level. Many third-party payers have specific coverage rules regarding what they consider medically necessary, or have riders and exclusions for specific procedures. Third-party payers may have a specific exclusion for procedures they consider experimental or unproven for a specific diagnosis or procedure, and it is imperative practices understand the protocols for billing a service.
For additional information or questions on coding, billing and auditing, contact Antanya Chung, CPC, CPC-I, CRHC, CCP, at [email protected].