New Genetic Insights in the Pathogenesis of CVID
It has long been known that CVID also has a genetic component. While most cases of this disease occur sporadically, in 10% to 20% of CVID cases, at least one additional family member either suffers from CVID or selective IgA deficiency.9 With a ratio of about 4 to 1, autosomal dominant inheritance is more common than recessive inheritance in CVID families. Genetic linkage studies have revealed that the genetic defect involved in this disease cannot be reduced to a single gene locus.
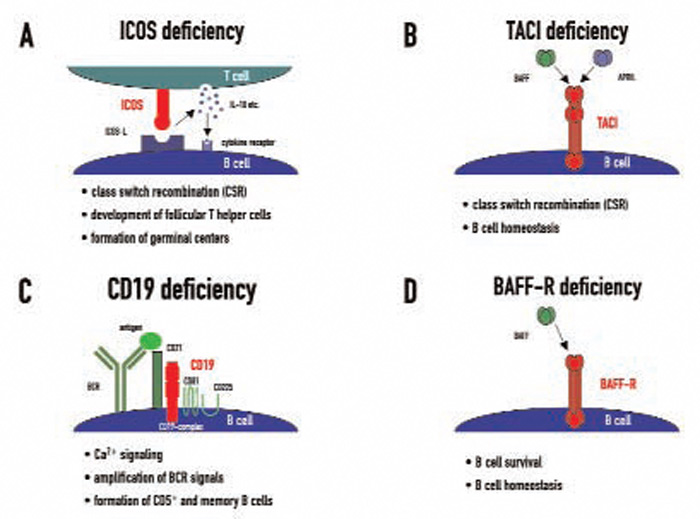
Candidate loci for CVID have now been demonstrated at the HLA region on chromosome 6, chromosome 4q, and chromosome 16q. This genetic heterogeneity—which probably mirrors the variable clinical presentation of this disease—is further increased by the recent discovery of four candidate genes which were found to be mutated in CVID independently of the results of previous linkage and association studies. These genes—ICOS, TACI, CD19, and BAFFR—encode for cell surface receptors on lymphocytes that play crucial roles either in peripheral B cell development or in B cell function.9