click for large version
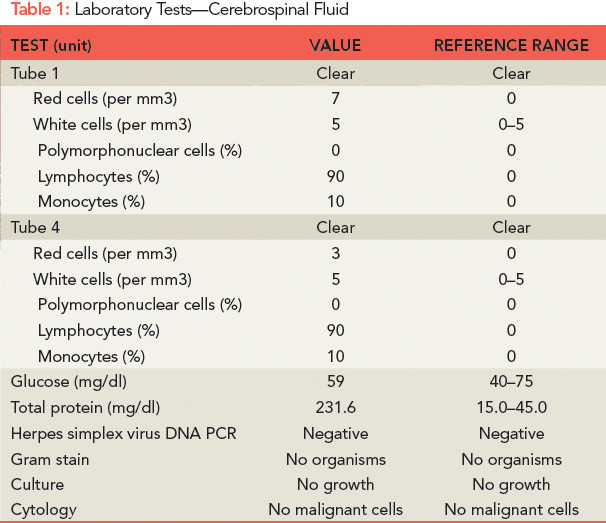
Table 1: Laboratory Tests—Cerebrospinal Fluid
SG was then transferred to our hospital for further evaluation. On arrival, he was afebrile and vital signs were normal. On neurologic examination, he was fully oriented, but was unable to relay his history due to word-finding difficulties, and speech was fragmented and circumferential in nature. He was able to recall zero out of three objects at five minutes. His cranial nerves were intact, but he had decreased hearing in the right ear. His reflexes were equal and intact. Mild dysmetria was observed with his left upper and lower extremities. His gait was unstable and he could not walk in tandem. His behavior was disinhibited and he expressed paranoid and delusional thoughts.

