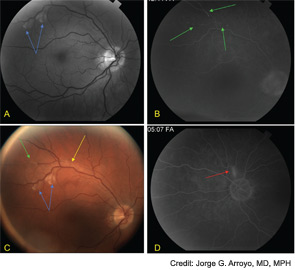
Figure 2: Fluorescein angiography reveals cotton wool spots (blue arrows), box-carring (yellow arrows), and peripheral retinal arteriolar branch occlusions (green arrows) in the right eye (A-C) and a focally inflamed retinal arteriole (red arrows) in the left eye (D).
Fluorescein angiography of the retina often shows hyperfluorescence of the wall of the retinal arterioles, and complete occlusion of distal branches.16 The occlusions may be associated with Gass plaques, atheromatous deposits caused by leakage of lipids into the arterial wall at the site of damage.16 Cotton wool patches and boxcar segmentation may also be seen, as was seen in our patient. Pathologic analysis of the retina have demonstrated serous deposits, with compression of retinal vessel lumens, no thrombosis, and decreased adenosine diphosphatase (ADPase) activity suggesting endothelial cell dysfunction and vaso-occlusion.17 Patients do not have visual loss when the occlusions spare the macula.

