Factors Associated with Depression in RA
Considerable research has been conducted on the variables associated with depression in RA.8 Although it has long been known that arthritis is associated with psychiatric comorbidity, an important question is whether having arthritis increases the risk of developing depression, or whether depression increases the odds of developing arthritis. A large, epidemiological study conducted in the Netherlands in which patients were sampled in their homes revealed that having arthritis (of any type) significantly increased the odds of developing depression two years later, while prior depression had no effect on the development of arthritis.9 Although the study did not address the factors or mechanisms associated with arthritis that led to this outcome, the significance of this study is that it highlighted the potential impact of arthritis on the emotional functioning of patients residing in the community. For many years, a central issue related to impact of arthritis has concerned the relative influence of disease activity versus psychosocial factors in explaining depression.
A biopsychosocial perspective examining the conjoint influence of multiple factors has been the dominant paradigm for studying depression in RA among behavioral medicine researchers.10 Much of this research has focused on the contributions of disease activity, pain, and disability to mood disturbance. Many studies have shown that heightened disease activity, pain, and disability may lead to depression.11 However, in addition to the independent effects of these variables, cyclical, synergistic relationships among these factors may partly explain their impact on depression. One scenario posits disability may be the final common pathway through which these other factors affect depression. For example, high disease activity may give rise to pain that creates impairments in functioning, including disability. Disability, in turn, may contribute to depression by interfering with mobility, performance in social roles, or by limiting the ability to engage in meaningful or valued life activities. Once mood deteriorates, patients may struggle to cope with their pain and self-manage their condition, further perpetuating this downward spiral.
Another way to view the impact of disease-related factors is to consider them as risk factors, not as actual determinants of depression in RA. The rationale for this perspective is that psychological factors also have been shown to affect depression and may either mitigate or exacerbate the effects on disease characteristics. For example, illness beliefs may affect the interpretation of symptoms and disease course and reflect the underlying meaning to patients of being sick or incapacitated by their medical circumstances. For instance, considerable research over the past 25 years has shown that the perception of helplessness in the face of pain or heightened disease activity plays a central role in depression in RA.12 Likewise, catastrophizing—the tendency to have dire thoughts about pain or the consequences of RA—may contribute to both depression and anxiety.13
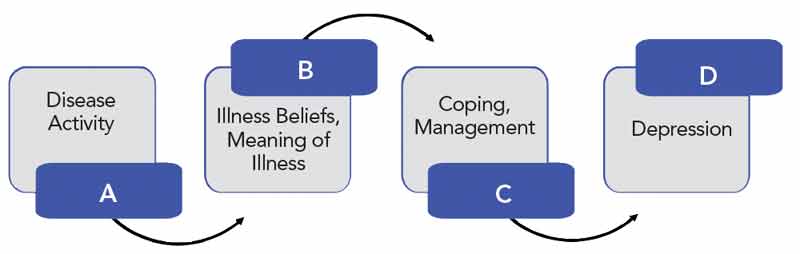
Dysfunctional beliefs about RA may also lead to maladaptive coping that, in turn, contributes to depression. For example, helplessness has been associated with passive or avoidant pain coping strategies that negatively impact mood.14 In contrast, internality (perception of control) is related to active pain coping that tends to be protective of mood. Illness beliefs and coping mechanisms may serve as important explanatory links between disease activity and mood, functioning as mechanisms through which factors such as pain and/or disability lead to depression and emotional distress (see Figure 1). The implication of this model is that treating disease activity is insufficient for the amelioration of depression. Emphasizing the implementation of strategies to correct dysfunctional beliefs or improve pain coping mechanisms may lead to improvement in mood.
Health Consequences of Depression
The presence of depression, due either to a previous or ongoing depressive disorder or the impact of having RA, may have far-reaching health-related consequences. Depression can lead to considerable suffering and impairment for afflicted patients.
Depression in RA has been associated with increased mortality and risk for comorbidities. For example, Ang and colleagues found that among a cohort of RA patients followed for four years, those with recurrent depression were at least twice as likely to die compared with those patients who were not depressed.15 Scherrer and colleagues examined whether depression is a risk factor for incident myocardial infarction in a sample of RA patients from a VA medical setting.16 Depressed patients were found to have a 40% increased risk of having a heart attack compared to nondepressed patients. These findings are consistent with studies from other medical populations showing increased risk for myocardial infarction among depressed patients.17 A variety of factors could serve as potential mechanisms linking depression with such health risks, including inflammation, poor adherence, or maladaptive health behaviors. However, research has not been conducted to identify these explanatory mechanisms in RA.
Depression may also aggravate RA symptoms and lead to impairment in important functional outcomes. Research has demonstrated that depression contributes to sleep disturbance and has been shown to mediate the effects of pain on poor sleep quality.18 When pain increases, depression worsens and interferes with sleep. Independent of the effects of inflammation and disease activity, depression has been correlated with greater fatigue and pain, unemployment and work disability, and impairments in quality of life and role functioning.19-21 A large, longitudinal study conducted by Morris and colleagues found that, over time, depressed RA patients had significantly poorer functional outcomes, including disability, and self-rated health than nondepressed patients.22 Depression may also lead to marital conflict, reduce the size of patients’ social network, and inhibit the receipt of social support. Negative social consequences of depression, in turn, can lead to greater depression and poorer emotional functioning.23
Moreover, there is significant evidence that depression leads to increased health-care seeking, contributing to unnecessary medical visits, procedures, and expensive treatments.5 Brief behavioral interventions that contribute to adaptive health functioning and reduce depression may lessen the deleterious impact of RA and lower medical costs.24
Clinical Management of Depression in Rheumatology
Rheumatologists face the responsibility and challenge of addressing depression in their clinical interactions with patients. Despite potential service delivery barriers, the outlook for managing depression in RA patients is positive. A major reason for optimism is that depression is a treatable disorder. Extensive research over the past 30 years has documented the efficacy of pharmacological, psychological, and behavioral treatments for depression.25 Empirically validated diagnostic procedures for identifying and managing depression can be implemented to augment the health and well-being of depressed patients with RA. A recurrent problem is that such procedures are not routinely implemented in rheumatology practice, thus perpetuating the existence of an important service delivery gap in clinical care.
Depression can be easily identified in rheumatology practice. Screening mechanisms can be integrated into the evaluation process and used intermittently to assess depression over the course of managing patients’ disease activity and response to medications. Brief self-report instruments such as the Patient Health Questionnaire (also known as the PHQ9) can be completed within a few minutes and provide cutoff scores that have high specificity and sensitivity for detecting depressive disorder.26 The clinician can use the data to alter the treatment plan for a patient and determine whether the depression should be treated.
After depression has been identified, the rheumatologist must decide on a management approach. If the patient’s depression is mild and does not impair role functioning, some basic education about depression and treatment provided by the rheumatologist or a rheumatology nurse may be sufficient. However, if the patient is likely to have a depressive disorder, consultation with a mental health professional is necessary to arrive at a definitive diagnosis and establish a management approach. Behavioral medicine specialists, either PhD clinical psychologists or psychiatrists who have training in understanding the relationship between psychological factors and chronic disease, are the most qualified to serve RA patients with depression and to coordinate their treatment with rheumatology professionals.
The high prevalence of depression in RA increases the importance of adopting an integrated approach to clinical management in which the medical and psychosocial needs or patients are effectively addressed and managed on a continuous basis. This approach, espousing a comprehensive view of the health of the RA patient, holds the most promise to yield optimal medical and psychological outcomes in rheumatology care.
Dr. Nicassio is clinical professor in the department of psychiatry at David Geffen School of Medicine at the University of California, Los Angeles. Myra Irani is with the California School of Professional Psychology, Los Angeles, at Alliant International University.
References
- Covic T, Tyson G, Spencer D, et al. Depression in rheumatoid arthritis patients: Demographic, clinical, and psychological predictors. J Psychosom Res. 2006;60:469-476.
- Escalante A, Rincon I, Mulrow CD. Symptoms of depression and psychological distress among Hispanics with rheumatoid arthritis. Arthritis Care Res. 2000;13:156-167.
- Margaretten M, Barton J, Julian L, et al. Socioeconomic determinants of disability and depression in patients with rheumatoid arthritis. Arthritis Care Res. 2011;63:240-246.
- Sleath B, Chewning B, de Vellis BM, et al. Communication about depression during rheumatoid arthritis patient visits. Arthritis Rheum. 2008;15:186-191.
- Joyce AT, Smith P, Khandker R, et al. Hidden cost of rheumatoid arthritis (RA): Estimating cost of comorbid cardiovascular disease and depression among patients with RA. J Rheumatol. 2009;36:743-752.
- Nicassio PM. The problem of detecting and managing depression in the rheumatology clinic. Arthritis Care Res. 2008;59:155-158.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed.). 2000. Arlington, VA: American Psychiatric Association.
- Dickens CA, McGowan L, Clark-Carter D, et al. Depression in rheumatoid arthritis: A systematic review of the literature with meta-analysis. Psychosom Med. 2002;64:52-60.
- Van’t Land H, Verdurmen J, Ten Have M, et al. The association between arthritis and psychiatric disorders; results from a longitudinal population-based study. J Psychosom Res. 2010;68:187-193.
- Engel GL. The clinical application of the biopsychosocial model. Am J Psychiatry. 1980;137:535-544.
- Brown G. A causal analysis of chronic pain and depression. J Abnorm Psychol. 1990;99:127-137.
- Nicassio PM, Wallsston KA, Callahan LF, et al. The measurement of helplessness in rheumatoid arthritis: The development of the arthritis helplessness index. J Rheumatol. 1985;12:462-467.
- Edwards RR, Cahalan C, Mensing G, et al. Pain, catastrophizing, and depression in the rheumatic diseases. Nat Rev Rheumatol. 2011;7:216-224.
- Brown GK, Nicassio PM. Development of a questionnaire for the assessment of active and passive coping strategies in chronic pain patients. Pain. 1987;1:53-74.
- Ang DC, Choi H, Kroenke K, et al. Comorbid depression is an independent risk factor for mortality in patients with rheumatoid arthritis. J Rheumatol. 2005;32:1013-1019.
- Scherrer JF, Virgo KS, Zeringue A, et al. Depression increases risk of incident myocardial infarction among veterans administration patients with rheumatoid arthritis. General Hosp Psychiatry. 2009;31:353-359.
- Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation. 1995;91:999-1005.
- Nicassio PM, Ormseth SR, Kay M, et al. The contribution of pain and depression to self-reported sleep disturbance in patients with rheumatoid arthritis. Pain. 2012;153:107-112.
- Nicassio PM, Ormseth SR, Custodio M, Irwin MR, Olmstead R, Weisman MH. A multidimensional model of fatigue in patients with rheumatoid arthritis. J Rheumatol. 2012;39:1807-1813.
- Lowe B, Willand L, Eich W, et al. Psychiatric comorbidity and work disability in patients with inflammatory rheumatic diseases. Psychosom Med. 2004;66:395-402.
- Michaed K, Wolfe F. Comorbidities in rheumatoid arthritis. Best Practices Res Clin Rheumatol. 2007;21:885-906.
- Morris A, Yelin EH, Panopalis P, et al. Long-term patterns of depression and associations with health and function in a panel study of rheumatoid arthritis. J Health Psychol. 2011;16:667-677.
- Subodh BN, Avashi A, Chakrabarti S, et al. Psychosocial impact of dysthymia: A study among married patients. J Affect Disord. 2008;109:199-204.
- Dixon KE, Keefe FJ, Scipio CD, et al. Psychological interventions for arthritis pain management in adults: A meta-analysis. Health Psychol. 2007;26:241-250.
- Cuijpers P, Andersson G, Donker T, et al. Psychological treatment of depression: Results of a series of meta-analyses. Nord J Psychiatry. 2011;65:354-364.
- Gilbody S, Richards D, Brealey S, et al. Screening for depression in medical settings with the patient health questionnaire (PHQ): A diagnostic meta-analysis. J Gen Int Med. 2007;22:1596-1602.
