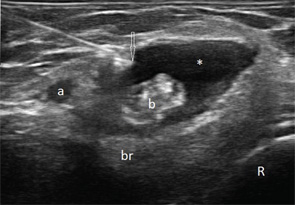
Figure 1
Transverse (see Figure 1) and longitudinal (see Figure 2) ultrasound images show an anechoic collection (asterisks),
Bicipitoradial bursitis can result from repetitive mechanical trauma, overuse, distal biceps tendon tear, tuberculosis,
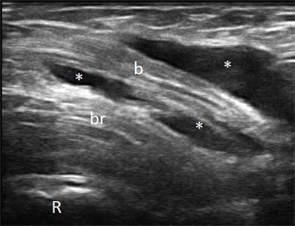
Figure 2
inflammatory arthritis, synovial chrondromatosis or amyloidosis. In our case the fluid was noninflammatory and crystal negative. Gram stain and culture, AFB smear and culture, cytology and Congo red stain were negative. The most likely reason for the bursitis remained overuse. Her symptoms improved with steroid injection and rest. Rarely, severe cases of bicipitoradial bursitis may require surgical resection of the bursa.
Ultrasound is useful in identifying bursitis, provides guidance for aspiration and injection, and allows for assessment of bicep tendon tear and macroscopic radial nerve damage resulting from compression.
Veronika Sharp, MD, is a faculty rheumatologist at the Santa Clara Valley Medical Center (SCVMC) in San Jose and is an affiliated clinical assistant professor at Stanford University, Palo Alto, Calif. She is director of musculoskeletal (MSK) ultrasonography in rheumatology at SCVMC.
Midori Jane Nishio, MD, is a rheumatologist in Walnut Creek, Calif., and is a volunteer faculty at SCVMC in MSK ultrasonography.
Lily Kao, MD, is a rheumatologist in San Jose, Calif., and is a volunteer faculty at SCVMC in MSK ultrasonography.