X-ray of the left ankle.
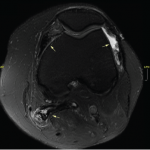
T1-weighted image of the left ankle.
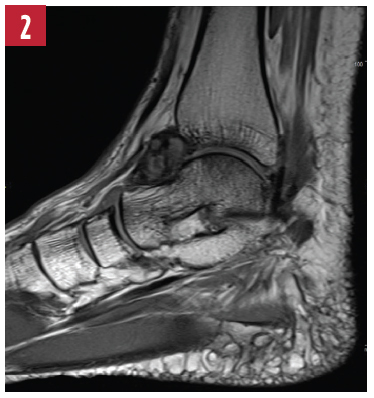
T2-weighted image of the left ankle.

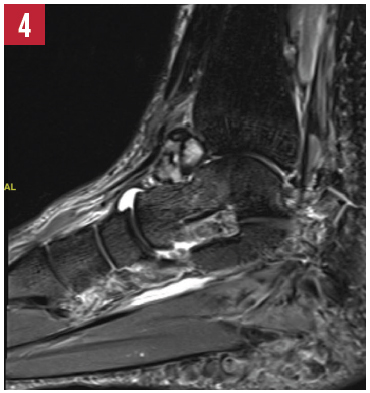
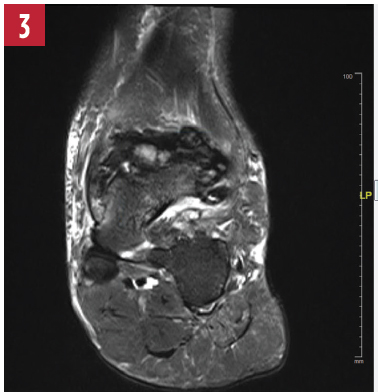
STIR image of the left ankle.

Cianna Leatherwood, MD, is a rheumatology fellow at Brigham and Women’s Hospital in Boston. Clinical and research interests include SLE and healthcare disparities.

Derrick J. Todd, MD, PhD, is a staff rheumatologist at Brigham and Women’s Hospital in Boston, and director of the Brigham and Women’s Rheumatology Musculoskeletal Ultrasound Center. Areas of clinical expertise include MSK ultrasound and adolescent rheumatology for patients transitioning from pediatric to adult rheumatology care.
References
- Chin KR, Barr SJ, Winalski C, et al. Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am. 2002 Dec;84-A(12):2192–2202.
- Kramer D, Frassica F, Frassica D, Cosgarea A. Pigmented villonodular synovitis of the knee—diagnosis and treatment. J Knee Surg. 2009 Jul;22(3):243–254.