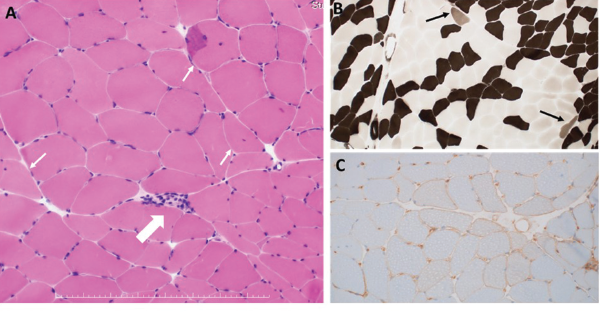
Figure 1: Histopathological Findings of Left Biceps Brachii
A: HE staining. One necrotic fiber was observed (large arrow). Some muscle fibers with internal nuclei were observed (small arrow). B: ATPase staining. A few type 2C fibers were observed (arrows). C: MHC Class I staining. Moderate upregulation of sarcolemmal MHC class I molecule was seen.
A diagnosis of immune-mediated necrotizing myopathy associated with these two antibodies was made. We started 50 mg a day of prednisolone orally, as well as cessation of mushroom intake. His symptoms and CK levels quickly improved. We tapered the prednisolone and started azathioprine. Although we discontinued azathioprine because of side effects, his symptoms remained stable. Eighteen months later, we successfully discontinued prednisolone and are now observing his symptoms without treatment.
In East Asia, the rate of statin-naive, anti-HMGCR antibody-positive immune-mediated necrotizing myopathy is much higher than in North America, raising a possibility that different triggering materials may be associated with immune-mediated necrotizing myopathy.
Discussion
Statins are believed to trigger autoantibody production against HMGCR in individuals who have a susceptibility.8 Regenerating fibers are known to overexpress HMGCR. Therefore, statin-induced myofiber necrosis and generation may well provide more antigens to produce pathogenic autoantibodies, creating a feed-forward loop.2,7 The binding of statins to HMGCR may also change the conformation of the protein, leading to the generation of new epitopes to which the immune system is not tolerant.2
In East Asia, the rate of statin-naive, anti-HMGCR antibody-positive immune-mediated necrotizing myopathy is much higher than in North America, raising a possibility that different triggering materials may be associated with immune-mediated necrotizing myopathy—especially in patients in East Asia.3-5 In this regard, it may be an attractive hypothesis that the foods containing natural HMGCR inhibitors, such as shiitake mushrooms, red yeast rice and pu’erh tea (a variety of fermented tea), which are apparently consumed more frequently in the region, trigger the disease in this statin-naive population. Further, infantile-onset immune-mediated necrotizing myopathy associated with anti-HMGCR autoantibodies has been found in patients from Japan.6 This is interesting considering shiitake mushrooms are often used as a weaning food in Japan.


