Updates from the ACR Convergence 2023 Review Course, part 4

The Review Course drew quite the crowd on Saturday morning at ACR Convergence 2023.
SAN DIEGO—Under the leadership of moderators Noelle Rolle, MBBS, assistant professor in the Division of Rheumatology, associate program director of the Rheumatology Fellowship at the Medical College of Georgia, Augusta University, and Julia Schwartzmann-Morris, MD, associate professor, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Great Neck, N.Y., the one-day Review Course held before ACR Convergence 2023 officially kicked off on on Saturday, Nov. 11, covered a plethora of important topics.
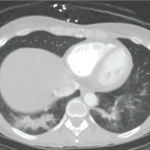
Relapsing Polychondritis
Marcela Ferrada, MD, who most recently was on faculty with the National Institutes of Health (NIH), Bethesda, Md., discussed relapsing polychondritis (RP), a condition that she herself has and for which she serves as a passionate advocate.