She continued to have worsening fatigue, myalgias and arthralgias involving the elbows and wrists, as well as left upper quadrant and left lower quadrant abdominal pain with fevers to 101.8ºF. Her labs were significant for worsening pancytopenia with leukopenia to 2.8 K/µL, thrombocytopenia to 58 K/µL and anemia with hemoglobin 5 g/dL. Additionally, it was noted that her ferritin increased to 1,197 ng/mL and her triglyceride increased to 560 mg/dL. She received three additional days of high-dose steroids with methylprednisolone 1,000 mg IV/day, and anakinra by subcutaneous injection (100 mg daily) was initiated. She again experienced worsening fatigue and night sweats when her steroids were transitioned to oral prednisone, so the dose of anakinra was increased to 200 mg daily.
Due to her persistent symptoms, there was concern that the driving force behind her HLH may not be AOSD as originally suspected. While this was being deliberated, her soluble interleukin (IL) 2 receptor alpha (sCD25 or sIL-2R) level was reported to be elevated to 9959. Past studies by Tsuji et al showed that the mean serum ratio of sIL2R:ferritin of patients with HLH secondary to lymphoma was found to be greater than the ratio in benign disease-associated HLH. Our patient’s serum ratio of serum soluble interleukin 2 receptor (sIL-2R):ferritin was markedly elevated at 8.3; therefore, malignancy-associated HLH was reconsidered despite her prior negative evaluation.
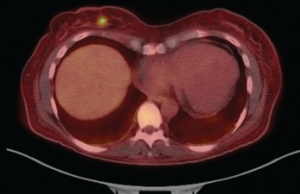
Figure 2: Fused PET-CT Image
The fused PET-CT shows the FDG-avid, right breast lesion measuring 7×4 mm, which is concerning for malignancy.
For further workup, she had a PET scan performed, which revealed an FDG-avid, 7 mm right breast lesion (see Figure 2). A mammogram showed an echogenic mass, concerning for malignancy. An ultrasound-guided core biopsy of this lesion revealed a diffuse large B cell lymphoma (see Figure 3), with the breast as the likely primary site (high-grade breast lymphoma). The neoplastic cells were found to be diffusely immunoreactive for CD20, co-expressed BCL6, BCL2 and MUM1, and were negative for CD10, CD43 and BCL1.
Soon after this diagnosis was established, she completed six cycles of intrathecal methotrexate with corticosteroids, EPOCH (etoposide, prednisolone, oncovin or vincristine, cyclophosphamide, hydroxydaunorubicin) and rituximab. Her symptoms, as well as her pancytopenia, resolved. Repeat PET scans over the past year have demonstrated no evidence of disease.
Discussion
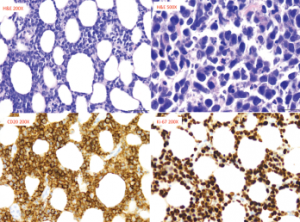
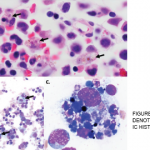
Figure 3: Pathology from Right Breast Core Biopsy
The biopsy revealed diffuse large B cell lymphoma, with neoplastic cells, which are diffusely immunoreactive for CD20. These cells also co-expressed BCL6, BCL2 and MUM1, but were negative for CD10, CD43 and BCL1.