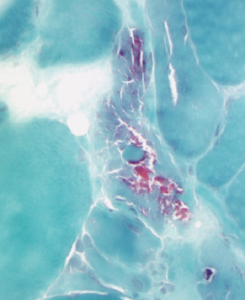
Figure 2B: This acid phosphatase stain of Patient 2’s muscle biopsy shows large numbers of necrotic fibers (highlighted in the center of the image).
Because our patient was in respiratory distress, we evaluated him for cardiac dysfunction and respiratory involvement. Transthoracic echocardiography showed 40% ejection fraction with mild to moderate left ventricular systolic and diastolic dysfunction. His chest CT demonstrated no evidence of interstitial lung disease (ILD), and his NIF measured <-15, highlighting significant respiratory muscle involvement. His arterial blood gas revealed hypoxic hypercapnic respiratory failure, and we intubated him after he failed a bilevel positive airway pressure (BiPAP) trial.
We started the patient on a combination of high-dose steroids and IVIG, because he had severe muscle weakness with profound respiratory muscle involvement leading to respiratory failure. During hospitalization, his weakness improved and his CPK levels trended down to 800 U/L. We continued him on steroids and monthly IVIG. On his follow-up visit two months later, his respiratory status and muscle strength had significantly improved.


