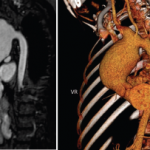
Vascular involvement can include both the venous and arterial systems. One-third of cases have thrombophlebitis of either the deep or the superficial veins, usually of the lower extremities. Despite the high frequency of thrombophlebitis, thromboembolism is rare, most likely due to the high adherence of thrombi to the diseased veins. Pulmonary arterial aneurysms are associated with a high mortality rate (See Figure 3, above right). The main symptom is hemoptysis, and patients with this symptom usually have associated thrombophlebitis.
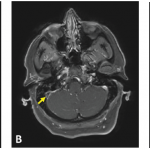
Central nervous system involvement occurs in 5% to 10% of patients and is one of the most serious manifestations of BS, causing increased rates of morbidity and mortality. Eighty percent of patients with CNS disease have parenchymal brain involvement. This mainly affects the brainstem and is manifested by pyramidal symptoms, followed by cerebellar and sensory symptoms and signs, sphincter disturbances, and behavioral changes. Nonparenchymal disease (observed in approximately 20% of those with CNS involvement), which is seen as intracranial hypertension due to dural sinus thrombosis, is manifested by headaches and papilloedema. Simultaneous involvement of the dural sinuses and brain parenchyma is unusual. Dural sinus thrombosis has a relatively benign prognosis in contrast to parenchymal involvement. Peripheral neuropathy, seen frequently in other vasculitides, is uncommon. In contrast, audiovestibular disease is increasingly recognized.
Although GI disease is frequent in up to one-third of BS patients from Japan and the U.S., it is quite rare among BS patients from Turkey. Symptoms include anorexia, vomiting, dyspepsia, diarrhea, and abdominal pain. Mucosal ulceration is most commonly seen in the ileum, followed by the cecum and other parts of the colon. Ileocecal ulcers have a distinct tendency to perforate. It can difficult to differentiate inflammatory bowel disease from BS histologically. Therefore, the rarity of rectal involvement and fistulas in BS is a helpful feature.
Unlike many other systemic vasculitides, glomerulonephritis is uncommon. Amyloidosis of the AA type is seen sporadically. Epididymitis is seen approximately 5% to 10% of patients.
TABLE 1: International Study Group Diagnostic (Classification) Criteria for BS*6
Recurrent oral ulceration: Minor aphthous, major aphthous, or herpetiform ulceration observed by physician or patient recurring at least three times in a 12-month period.
Plus two of the following symptoms:
- Recurrent genital ulceration: Aphthous ulceration or scarring, observed by physician or patient.
- Eye lesions: Anterior uveitis, posterior uveitis, cells in the vitreous detected with slit-lamp examination, or retinal vasculitis observed by ophthalmologist.
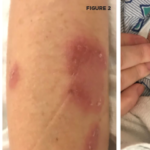
- Skin lesions: Erythema nodosum observed by the physician or patient, pseudofolliculitis, papulopustular lesions, or acneiform nodules observed by physician in postadolescent patients not on corticosteroid treatment.
- Pathergy: Read by physician at 24 to 48 hours.
*Findings applicable only in the absence of other clinical explanations.