(Click for larger image)
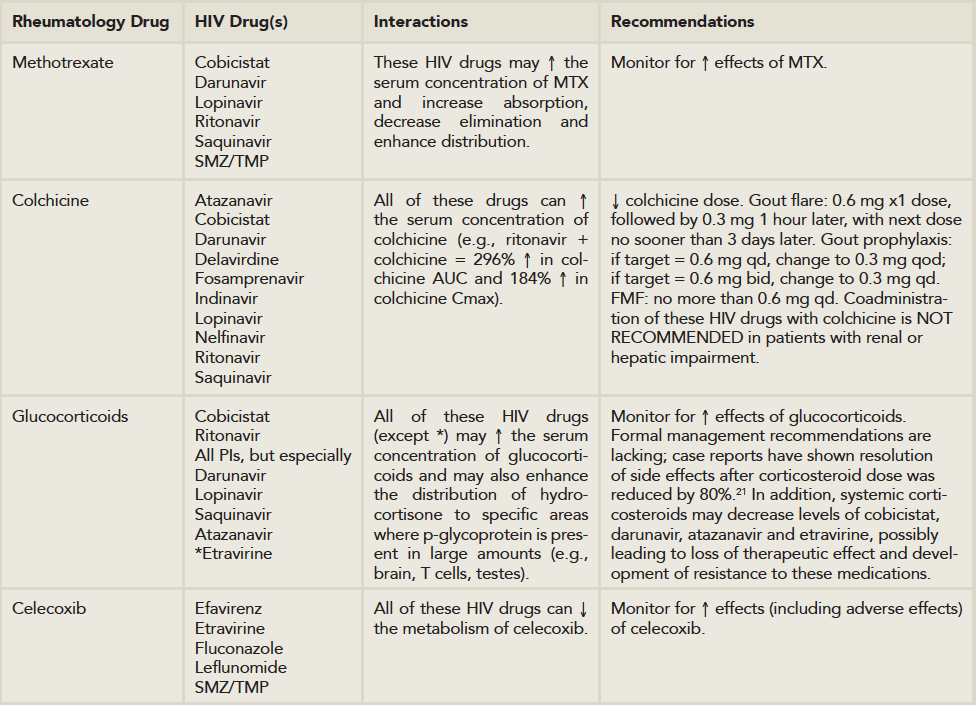
Table 2: Important Rheumatology/HIV Drug-Drug Interactions.
Source: Lexicomp Online, Interactions, Hudson, Ohio: Lexi-Comp Inc.; March 12, 2015
Numerous glucocorticoids use CYP3A4 as their major route of metabolism and, thus, are vulnerable to profound pharmacokinetic and pharmacodynamic fluctuations in the presence of these HIV drugs. The frequency and magnitude of these drug–drug interactions with glucocorticoids as a class are not well known, regardless of the route of administration (e.g., oral, intra or periarticular, inhaled as well as other routes).
For rheumatologists and advanced practitioners in rheumatology, extreme caution should be exercised when using glucocorticoids in patients on these HIV drugs. The situation appears most critical for our specialty with regard to the interaction of ritonavir and/or protease inhibitors with the administration of intrarticular or soft tissue triamcinolone, which has been reported to induce an iatrogenic hypercortisolism within a few weeks, as well as secondary adrenal insufficiency following a single injection. These cases have recently been reviewed.22 For oral administration of prednisone or prednisolone, no formal recommendations have been made for dose adjustment, although at the minimum, extreme caution should be exercised with their use (see Table 2). Most importantly, if new medications are contemplated in a patient with HIV infection already on therapy, a specific discussion about the possible ramifications should be had with the HIV caregiver.
 Leonard H. Calabrese, DO, is professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, in Cleveland, Ohio; the RJ Fasenmyer Chair of Clinical Immunology; the Theodore F. Classen, DO, Chair of Osteopathic Research and Education; and vice chairman of the Department of Rheumatic and Immunologic Diseases.
Leonard H. Calabrese, DO, is professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, in Cleveland, Ohio; the RJ Fasenmyer Chair of Clinical Immunology; the Theodore F. Classen, DO, Chair of Osteopathic Research and Education; and vice chairman of the Department of Rheumatic and Immunologic Diseases.
 Elizabeth Kirchner, MSN, CNP, is director of patient care for the R.J. Fasenmyer Center for Clinical Immunology and has been a nurse practitioner for 15 years in the Department of Rheumatic and Immunologic Diseases at the Cleveland Clinic in Ohio.
Elizabeth Kirchner, MSN, CNP, is director of patient care for the R.J. Fasenmyer Center for Clinical Immunology and has been a nurse practitioner for 15 years in the Department of Rheumatic and Immunologic Diseases at the Cleveland Clinic in Ohio.
References
- Kallings LO. The first postmodern pandemic: 25 years of HIV/AIDS. J Intern Med. 2008 Mar;263(3):218–243.
- Samji H, Cescon A, Hogg RS, et al. Closing the gap: Increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One. 2013;8(12):e81355.
- Centers for Disease Control and Prevention. HIV among older Americans. 2013.
- Deeks SG. HIV infection, inflammation, immunosenescence, and aging. Annu Rev Med. 2011;62:141–155.
- Weyand CM, Yang Z, Goronzy JJ. T-cell aging in rheumatoid arthritis. Curr Opin Rheumatol. 2013 Jan;26(1):93–100.
- Hunt PW. HIV and inflammation: Mechanisms and consequences. Curr HIV/AIDS Rep. 2012 Jun;9(2):139–147.
- Crowson CS, Liao KP, Davis JM 3rd, et al. Rheumatoid arthritis and cardiovascular disease. Am Heart J. 2013 Oct;166(4):622–628.e1.
- Winchester R, Bernstein DH, Fischer HD, et al. The co-occurence of Reiter’s syndrome and acquired immunodeficiency. Ann Intern Med. 1987 Jan;106(1):19–26.
- Lawson E, Bond K, Churchill D, et al. A case of immune reconstitution syndrome: Adult-onset Still’s disease in a patient with HIV infection. Rheumatology (Oxford). 2009 Apr;48(4):446–447.
- Patel N, Patel N, Espinoza LR. HIV infection and rheumatic diseases: The changing spectrum of clinical enigma. Rheum Dis Clin North Am. 2009 Feb;35(1):139–161.
- Nguyen BY, Reveille JD. Rheumatic manifestations associated with HIV in the highly active antiretroviral therapy era. Curr Opin Rheumatol. 2009 Jul;21(4):404–410.
- Calabrese LH, Kirchner E, Shrestha R. Rheumatic complications of human immunodeficiency virus infection in the era of highly active antiretroviral therapy: Emergence of a new syndrome of immune reconstitution and changing patterns of disease. Semin Arthritis Rheum. 2005 Dec;35(3):166–174.
- Gedmintas L, Solomon DH. HIV and its effects on bone: A primer for rheumatologists. Curr Opin Rheumatol. 2012 Sep;24(5):567–575.
- Miller KD, Masur H, Jones EC, et al. High prevalence of osteonecrosis of the femoral head in HIV-infected adults. [Authors’ note: See comments.] Ann Intern Med. 2002 Jul 2;137(1):17–25.
- McComsey GA, Tebas P, Shane E, et al. Bone disease in HIV infection: A practical review and recommendations for HIV care providers. Clin Infect Dis. 2010 Oct 15;51(8):937–946.
- French MA. HIV/AIDS: Immune reconstitution inflammatory syndrome: A reappraisal. Clin Infect Dis. 2009 Jan 1;48(1):101–107.
- Iordache L, Launay O, Bouchaud O, et al. Autoimmune diseases in HIV-infected patients: 52 cases and literature review. Autoimmun Rev. 2014 Aug;13(8):850–857.
- Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. Morbidity and Mortality Weekly Report., 2006 Sep 22;55(RR14):1–17.
- Harbell J, Terrault NA, Stock P. Solid organ transplants in HIV-infected patients. Curr HIV/AIDS Rep. 2013 Sep;10(3):217–225.
- Cepeda EJ, Williams FM, Ishimori ML, et al. The use of anti-tumour necrosis factor therapy in HIV-positive individuals with rheumatic disease. Ann Rheum Dis. 2008 May;67(5):710–712.
- Johnson SR, Marion AA, Vrchoticky T, Emmanuel PJ, Lujan-Zilbermann J. Cushing syndrome with secondary adrenal insufficiency from concomitant therapy with ritonavir and fluticasone. J Pediatr. 2006 Mar;148(3):386–388.
- Hall JJ, Hughes CA, Foisy MM, Houston S, Shafran S. Iatrogenic Cushing syndrome after intra-articular triamcinolone in a patient receiving ritonavir-boosted darunavir. Int J STD AIDS. 2013 Sep;24(9):748–752. Doi: 10.1177/09564462413480723.