HLA-B27 Assays
Although HLA-B27 is a genetic marker, the HLA-B27 status of a person can be determined using antibody-based cellular assays or with nucleic acid-based techniques (see Figure 2). The original method for HLA typing, which is still being used by some histocompatibility testing laboratories, was a cytotoxicity assay with monospecific sera from HLA-sensitized individuals and cells from the test subject. The binding of polyclonal anti-HLA-B27 antibodies present in these sera to HLA-B27 proteins on the cell surface results in complement-mediated lysis, which can be read out using a cell viability stain.
(click for larger image)
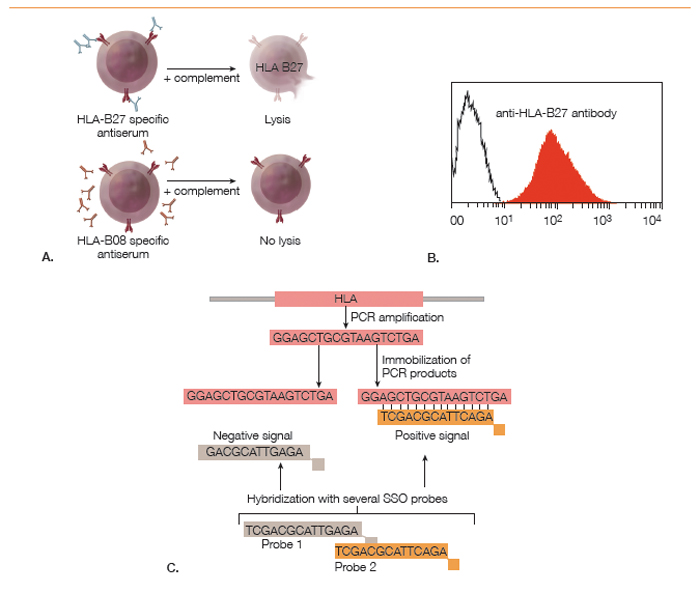
Figure 2: Methods for Determining HLA-B27 Status: A. Cytotoxicity assay using polyclonal monospecific antisera from sensitized humans; B. Flow cytometry analysis of cells stained with a fluorescently labeled monoclonal anti-HLA-B27 antibody; C. Polymerase chain reaction–sequence specific oligomerization (PCR-SSO). PCR amplification of the polymorphic exon is followed by hybridization with fluorescently labeled oligonucleotide probes to determine subtype identity.
The development of monoclonal antibodies has made HLA-B27 determination by flow cytometry feasible. In this method, peripheral blood cells from the test subject are incubated with a fluorescently labeled monoclonal antibody against HLA-B27. As MHC class I molecules are expressed on all cells, HLA-B27 positivity causes a fluorescence intensity shift of all cells relative to unstained cells or HLA-B27 negative control cells.


