Further, the constant stream of data allowed us to actually perform the “S” (study) part of the PDSA methodology, studying the impact of our changes in real time and using those data to inform subsequent interventions.
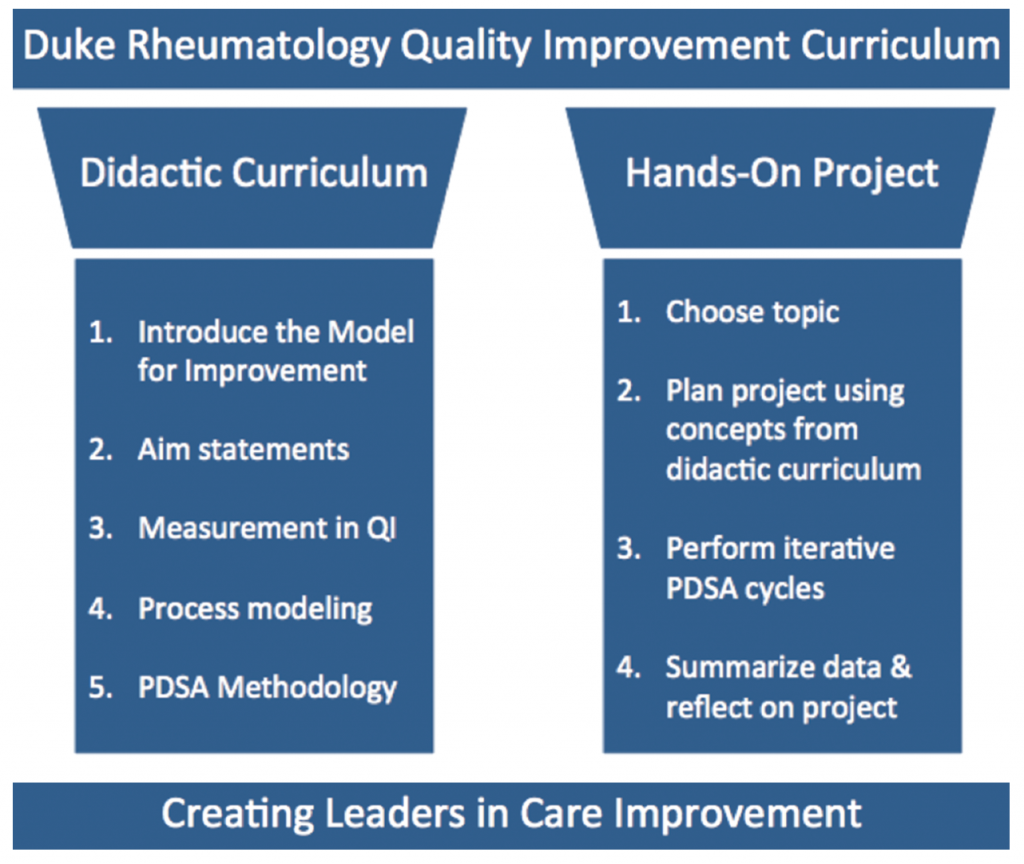
Figure 1: 2 Pillars of Success for the Duke Rheumatology Quality Improvement Curriculum
Moving forward, the objective of our QI curriculum continues to be developing rheumatologists with sufficient knowledge and experience to lead QI efforts in their future practice. This goal is balanced, but not eclipsed, by the desire to use the quality curriculum to make real improvements in our clinical practice.
Our curriculum remains based in the Institute for Healthcare Improvement (IHI) Model for Improvement, and we continue to provide a didactic series on that methodology, combined with real-world application in a yearly, fellow-led QI project (see Figure 1).
As modern medicine inches closer to the realities of value-based care, our fellows are being trained in the use of data science and learning health principles to analyze practice patterns in sustainable ways.
One doesn’t have to look far to see the value of this type of training. The RISE registry is gaining momentum, the ACR continues to develop quality measures for rheumatology practice, and legislators continue to debate the implementation of various quality incentive programs. Meanwhile, patients continue to suffer from medical errors, outdated practices, system inefficiencies, treatment delays, insufficient care and overtreatment. Upon graduation, our fellows will be ready to engage these issues and lead quality improvement initiatives for the betterment of patient care.


