Background/Purpose
It has been reported that 20–50% of patients with polymyalgia rheumatica (PMR) have subclinical giant cell arteritis (GCA). The natural history of ultrasound-defined subclinical GCA in PMR is not known.
Methods
Twenty-five newly diagnosed PMR patients who met a clinical diagnosis for PMR, verified by two rheumatologists, were examined by ultrasound. All six branches of the superficial temporal arteries and both axillary arteries were examined using a GE P9 device. Sonographic abnormalities considered indicative of vasculitis in the temporal arteries included the halo sign (see Figure 1) and non-compressible arteries with a thickened intima-media complex. In the axillary arteries, a halo sign and an intima-media thickness of >1.0 mm was considered positive. Follow-up consultations after one year were undertaken to review the clinical diagnoses.
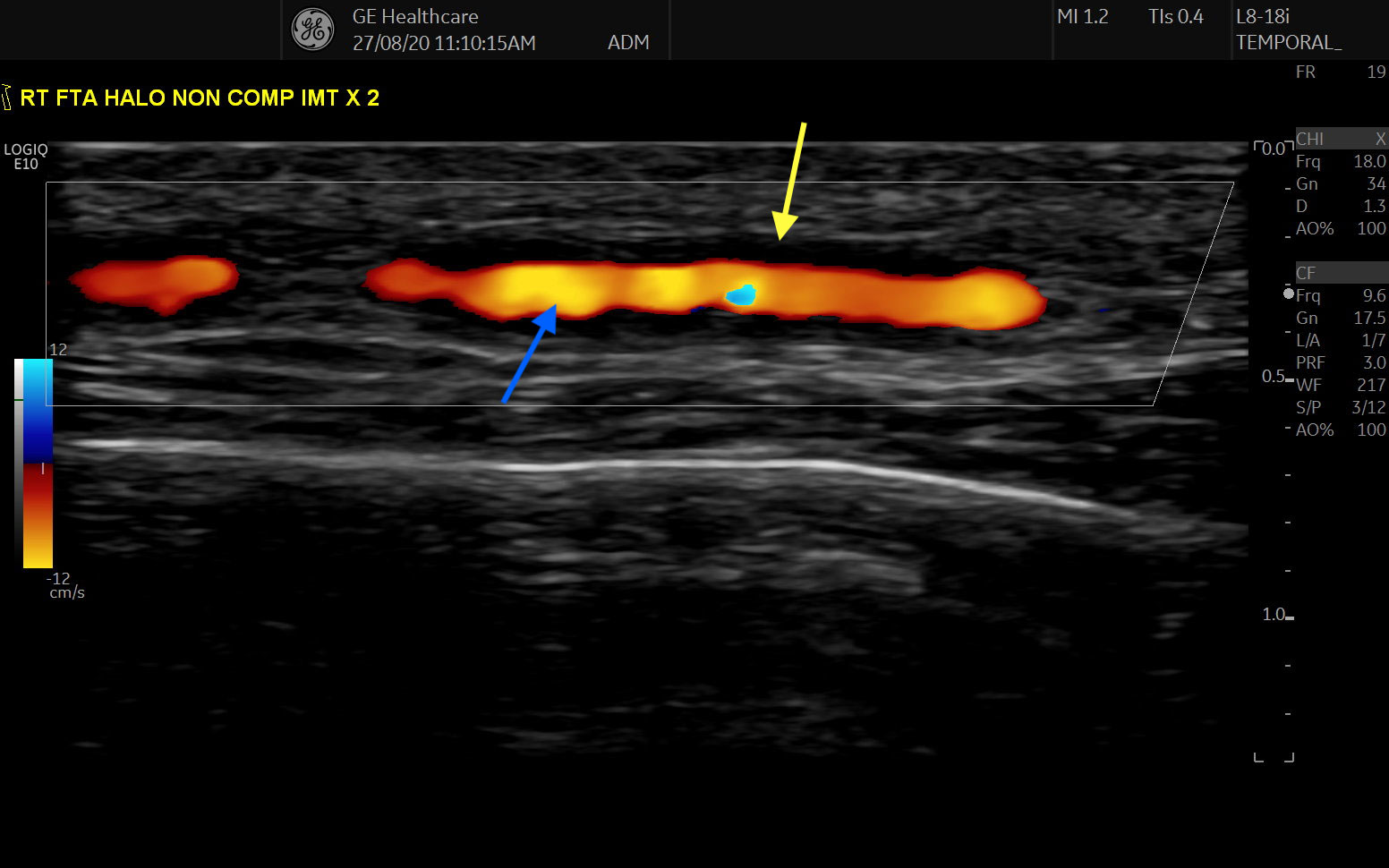
FIGURE 1: Longitudinal view of the frontal branch of the superficial temporal artery, demonstrating a halo sign, as indicated by the anechoic region (yellow arrow) surrounding the inner Doppler (blue arrow) signal. (Click to enlarge.)
In the subclinical GCA group (identified on ultrasound), a PMR-dose steroid taper was used, with a prompt clinical response; a GCA-dose steroid taper was initiated for those who subsequently flared; and tocilizumab was initiated in the event of a second flare.
Results
The cohort consisted of 64% women (n=16) with a mean age of 67 years (range 50–84). 2012 ACR/EULAR classification criteria were met in 16 of 25 patients (primarily due to prior corticosteroid use in primary care, resulting in a normal erythrocyte sedimentation rate [ESR] and C-reactive protein [CRP]).


