Her cutaneous disease was refractory to multiple medications. Systemic therapies included 400 mg of hydroxychloroquine by mouth daily, 25 mg of subcutaneous methotrexate weekly and 1,500 mg of mycophenolate mofetil by mouth twice daily. Adjunctive topical corticosteroids and topical calcineurin inhibitors were ineffective. She had required prednisone since diagnosis, with doses ranging from 5 mg to 60 mg by mouth daily. When the prednisone was tapered below 10 mg by mouth daily, cutaneous disease flared.
Clinical Findings
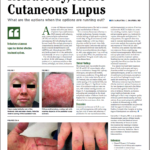
The physical exam was notable for active ACLE and SCLE lesions despite adherence to combination therapy with hydroxychloroquine, mycophenolate mofetil, methotrexate, prednisone 10 mg daily and topicals. A classic malar butterfly rash of the forehead, chin and malar cheeks, with relative sparing of the nasolabial folds, was present (see Figure 1). Significant involvement of the posterior scalp and ears was seen, with residual scarring alopecia (see Figure 2). A maculopapular, erythematous and scaling rash presented on the dorsal and palmar surfaces of bilateral hands (see Figures 3 & 4). These photographs were obtained at her most recent clinic visit.

Figures 1 & 2. Classic malar butterfly rash of the forehead, chin and malar cheeks. Note the relative sparing of the nasolabial folds.
Discussion
Cutaneous involvement in SLE is common and heterogeneous, with rashes ranging from mild to severe and refractory. A predilection for sun-exposed areas exists, and photosensitivity is common. First-line treatment for ACLE includes sun protection, smoking cessation, topical therapies and antimalarial agents (e.g., hydroxychloroquine, chloroquine and quinacrine). For many patients, this approach alone may result in dramatic improvement, with one recent meta-analysis demonstrating significant response in 91% of ACLE cases.1
However, some patients may have refractory cutaneous disease, requiring augmented immunosuppression. Methotrexate and mycophenolate mofetil are both reasonable second-line treatment options. Azathioprine may also be considered, but is generally less efficacious than the aforementioned treatments.2
Our patient tried and failed maximum doses of both methotrexate and mycophenolate mofetil on a background of hydroxychloroquine, as well as a brief trial of combination methotrexate, mycophenolate mofetil and hydroxychloroquine with careful lab monitoring for toxicity.

Figures 3 & 4 A maculopapular erythematous, violaceous, scaling rash is evident on the dorsal and palmar surfaces of both hands.
Refractory cutaneous lupus has limited effective treatment options.
Refractory cutaneous lupus has limited effective treatment options. Consensus on the best therapeutic approach after failure of second-line agents is limited by low levels of evidence. However, as rheumatology health professionals, we are challenged to find a way to improve quality of life and permit steroid-sparing for these patients. In an expert perspective published in Arthritis & Rheumatology in 2020, lenalidomide is recommended as a potential third-line agent for refractory cases.2 Studies of several other therapies at varying stages of development are underway.
More Info: See discussion with a dermatologist on this case here.
Samantha C. Shapiro, MD, is an academic rheumatologist and an affiliate faculty member of the Dell Medical School at the University of Texas at Austin. She received her training in internal medicine and rheumatology at Johns Hopkins University, Baltimore. She is also a member of the ACR Insurance Subcommittee.
References
- Chasset F, Bouaziz J-D, Costedoat-Chalumeau N, et al. Efficacy and comparison of antimalarials in cutaneous lupus erythematosus subtypes: A systematic review and meta-analysis. Br J Dermatol. 2017 Jul; 177(1):188–196.
- Borucki R, Werth VP. Expert perspective: An evidence‐based approach to refractory cutaneous lupus erythematosus. Arthritis Rheumatol. 2020 Nov;72(11):1777–1785.