In 2016, she was being treated with nivolumab to maintain remission at another hospital. A few days after the first treatment, she developed diarrhea and a rash on both lower shins, but no workup or intervention was done at the time.
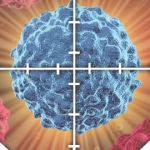
Two weeks later, the patient received her second cycle of nivolumab, with immediate worsening of the pretibial rash (see Figure 1). Seven days after that infusion, she presented at our institution with generalized fatigue, weakness and syncope. On initial evaluation, she was found to be bradycardic with a heart rate of 33 beats per minute. An electrocardiogram showed third-degree atrioventricular block. Laboratory data were remarkable for troponin levels of 27.3 ng/L (upper limit of normal [ULN] <0.6 ng/L]), creatine kinase (CK) levels of 6,322 IU/L (normal = 42-284 IU/L), CK-MB levels of 250 ng/dL (ULN<5.0 ng/dL), ALT levels of 182 u/L (normal = 4–36 IU/L) and AST levels of 247 u/L (normal = 13–39 IU/L).
The patient became hemodynamically unstable, and an emergent pacemaker was implanted. Her symptoms improved. Echocardiography revealed mild concentric left ventricular hypertrophy, mild mitral regurgitation, mild pulmonary hypertension and an ejection fraction of 55–60%. Cardiac catheterization showed multivessel disease that was stable when compared to results from the prior year. The cardiac catheterization excluded acute ischemic disease as the cause of the heart block, and no stent was placed. She received intravenous fluids. Her CK and troponin levels dropped to 3,000 IU/L and 16 ng/L, respectively. She also developed atrial fibrillation.
While the patient was hospitalized, she developed right eyelid droop and generalized weakness. A neurology assessment confirmed ptosis and 1 mm pupil asymmetry without other neurologic findings. Acetylcholine receptor antibody tests, and brain and spine imaging were negative. The working diagnosis was nerve infarct, aneurysm or myasthenia gravis.
The patient was prepared for discharge with a diagnosis of rhabdomyolysis and ischemia in the setting of cardiac hypoperfusion, and she was scheduled for outpatient cardiology and neurology follow-up. She was taken off the statin.
The patient returned to the hospital one week later with sudden onset shortness of breath, inability to clear phlegm, dysphagia, dysphonia and proximal upper and lower extremity muscle weakness and pain. She was unable to sit up in bed or stand. Prior to this, she had been walking two miles daily for exercise.
Laboratory analysis showed her cardiac and liver markers were still elevated and had actually been rising since her hospital discharge one week earlier: CK of 5,029 IU/L, CK-MB of 275 ng/dL, troponin of 6.2 ng/mL, ALT of 422 u/L and AST of 421 u/L.