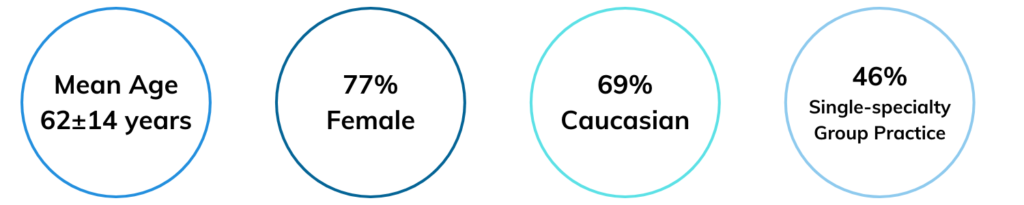
Figure 2: RISE registry demographic breakdown for rheumatoid arthritis patients. Data sourced from Izadi et al. findings.
“The fundamental challenge for RISE is that it was originally created for a specific purpose: to help practices survive in the Physician Quality Reporting System (PQRS) and pay-for-performance world,” says William Harvey, MD, MSc, FACR, clinical director of rheumatology and associate professor at Tufts University School of Medicine in Boston. Dr. Harvey serves as the chair of the ACR’s Committee on Research and Health Information Technology (RHIT). “We are now fighting against that built-in skew … our current data are not properly representative of all rheumatic patients. We are evolving our messaging to highlight how RISE is not just for federal reporting, but for clinicians interested in other aspects of our field, such as quality improvement, research and data to support health policy.”

Dr. William Harvey
Toward this end, the ACR is now taking additional steps to expand the diversity of RISE users and data. “We are now trying to use the data to learn something about the care of individuals and practices, and with that aim, we are diversifying the registry to have a more representative sample,” Dr. Harvey adds. “What we need now is for more practices to participate and share their data with the ACR—the more RISE users we have from diverse sections of the clinical world, the more robust RISE research findings and conclusions will be.”