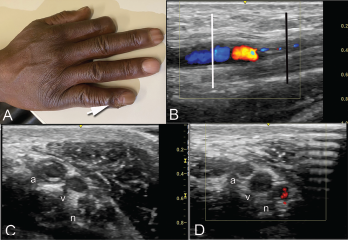
Clockwise from top: Image A shows the periungual ulceration (arrow) of the fifth digit, as well as the prior amputation of the second digit. Image B shows a longitudinal ultrasound of the palmar aspect of the ulnar right wrist. In the center of the image, the ulnar artery is in view and color Doppler flow is visualized within the vessel until there is a reversal of flow demonstrated by color change, followed by severe attenuation of flow distally. Distal to the cessation of flow, the vessel appears hypoechoic due to proliferation of the intima to the point of occluding the lumen. Image C shows a transverse view at the level of white line in Image B, with endothelial proliferation seen around a central lumen of the artery (a), next to the vein (v) and ulnar nerve (n). Image D, shows a transverse view at the level of the black line in Image B, where the arterial lumen (a) is occluded.
A 51-year-old man with a history of limited systemic sclerosis with Raynaud’s phenomenon and pulmonary hypertension being treated with tadalafil and macitentan presented to a clinic with ulceration of his right pinkie. The patient had injured the finger two months earlier. He reported poor healing and the presence of a persistent ulcer since the injury.
The patient had a history of a prior ulceration of the right index finger, which led to an amputation in 2011. He had no history of lower extremity vascular disease, diabetes mellitus or hypertension, but had smoked one pack of cigarettes per day for 20 years, quitting 10 years before.


