click for large version
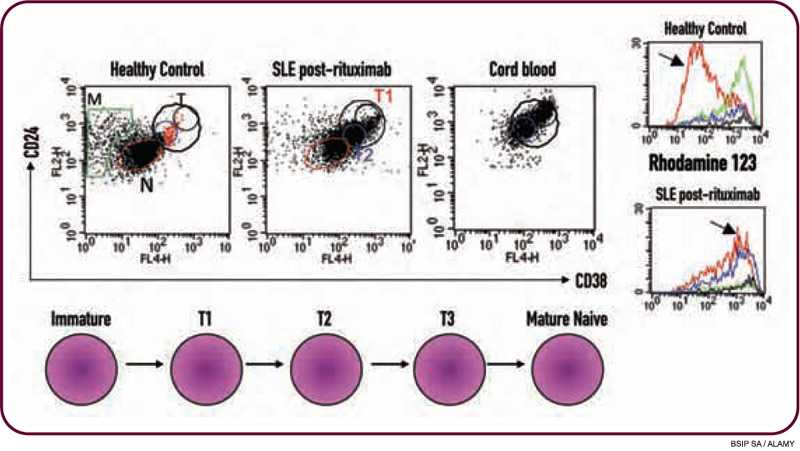
Figure 2: Long-term responders to B cell–depletion therapy in lupus display a unique B cell–reconstitution profile. Based on flow cytometry analysis, peripheral blood B cells from a healthy control are predominantly of a mature naive (N) phenotype with a small fraction of transitional (T) B cells, cells that are intermediate between immature in the bone marrow and mature in the periphery. In this SLE patient, after B-cell depletion and at the point of B-cell reconstitution, the majority of the peripheral B cells are of a transitional phenotype, similar to cord blood—in essence a “recapitulation of B-cell ontogeny.” Even the apparently mature naive B cells, based on lower expression of CD24 and CD38, are actually a T3 transitional B cell (see histogram for Rhodamine 123 extrusion at arrow).
Other B Cell–Targeted Therapies
