Patients with SLE may develop a wide array of neurologic features. GBS has appeared in a small number of SLE case reports. Patients with its acute form typically present with an ascending areflexic motor weakness without sensory loss. Others can present with a combination of sensory and/or motor findings (see Table 1). The MFS variant classically presents with the triad of ophthalmoplegia, ataxia and areflexia.
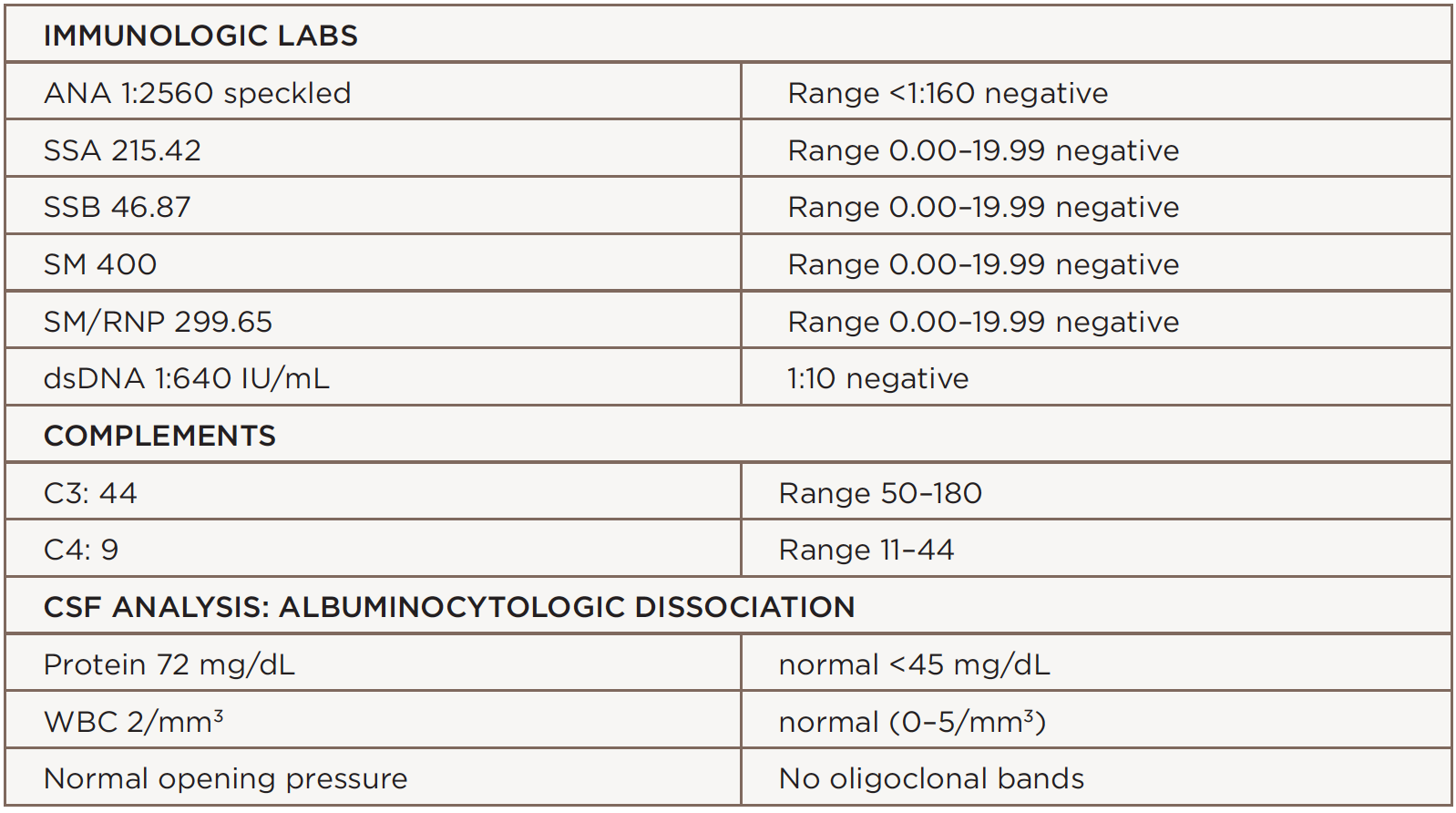
(click for larger image) Table 1: The patient’s immunologic labs & CSF Analysis
MFS is a rare GBS variant with ocular involvement. This subset is estimated to encompass 5–10% of GBS cases, with an incidence of one in 1 million. One-quarter of patients with MFS will develop extremity weakness in some form, which is the connecting factor to GBS. There may be incomplete presentations of MFS that present with different combinations, such as acute ophthalmoplegia without ataxia, or acute ataxic neuropathy without ophthalmoplegia. In addition, it is possible to see bulbar and facial weakness as presenting symptoms. Ophthalmoplegia in MFS is possibly the result of highly dense concentrations of GQ1b gangliosides, which are found in abducens, trochlear and oculomotor nerves. This imbalance of ganglioside antigenic targets results in anti-GQ1b antibodies binding to these ocular nerves causing damage leading to aberrant muscle function.6 anti-GQ1b antibodies appear in 85–90% of patients with MFS and may be a confirmatory finding.