These images illustrate the two MRI sequences that can be used together to diagnose spondyloarthritis in the sacroiliac joint, as described by Dr. Maksymowych. The T1-weighted MRI scan of the sacroiliac joint in the semi-coronal plane (top) is a fat-sensitive sequence, so subcutaneous fat appears bright. This scan is abnormal because it shows two large areas of bright signal in the sacrum adjacent to subchondral bone characterized by a homogeneous appearance and a distinct border.
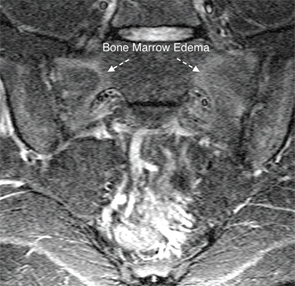
A STIR scan of the sacroiliac joint in the semi-coronal plane (bottom), taken from the same patient, is a water-sensitive scan with blood vessels and cerebrospinal fluid appearing bright. This scan is abnormal because it shows areas of bright signal in the subchondral bone marrow of the sacrum, a sign of bone marrow edema.
When both figures are viewed together, you can see that the area of bone marrow edema surrounds the area of fat metaplasia on the T1W scan—typical of inflammation that is resolving, but still remains active, in a patient with spondyloarthritis.
DICOM uses a large, uncompressed (5 to 10 megabyte) file format for medical images that are too large to send by email. It’s designed to allow consistent communication between scanners and the Picture Archiving and Communication System (PACS) that archives and allows retrieval of DICOM images. “DICOM viewers used by radiologists are too complicated for our purposes, and rheumatologists need something simpler. My organization, CaRE Arthritis, has developed a simplified DICOM viewer that is intuitive and doesn’t take very long to master,” he said.
Collaboration between Rheumatology & Radiology
Dr. Maksymowych strongly advocates that the rheumatologist and radiologist, who historically have occupied separate silos in healthcare, work together more closely. “The radiologist doesn’t see a lot of this particular condition, and rheumatologists, in their own silo, often don’t understand the role of MRI. They need to learn the terminology in order to have informed discussions with the radiologist,” he said. This application of MRI hasn’t been introduced into the rheumatology medical curriculum. “We don’t have trainees being exposed to the technology, and rheumatologist trainers aren’t familiar enough with it to teach it. So it becomes a vicious cycle,” he said.
