Recent reports noted that systemic symptoms were recorded in nearly one-third of the patients.2 Systemic MAP involves small- and medium-size arteries.5 Transformation from cutaneous to systemic can occur within months to years following the onset of dermatologic manifestations.6 Typically, around 30 skin lesions are seen in an average patient, but the presence of more than 600 has been described.7 Lesions may start as papules and persist as such, or they may develop a central area of necrosis that replaces the papule.8
The diagnosis is clinicopathologic because there are no specific laboratory tests.9
The most common cause of death is sepsis due to peritonitis and perforation (occurring in approximately 60% of reported cases) developing within two to three years of internal organ involvement.10
The etiology of MAP is unknown.11 Although there seems to be a genetic predisposition, no gene has been identified.11-13 MAP can be seen independently, or there may be MAP-like lesions seen in other connective tissue diseases (CTDs).6,10 There have been deposits consisting of activated complement pathway proteins, C5b-9, found in the tissues of patients with dermatomyositis, scleroderma and MAP.14-18 Dermal fibrosis can also be seen in each of these three diseases.17 A prior viral exposure has been theorized.14
MAP is a rare, life-threatening disease. With the most current findings & investigations, we may be able to bring some hope to patients—or at least open the door for further investigation.
History
MAP was first described by W. Köhlmeier, an Austrian physician, in 1941.2 Later, Robert Degos, MD, a French dermatologist, reported a 45-year-old plumber with typical MAP skin lesions who died of GI complications shortly after being diagnosed. At autopsy, the small intestine lesions were found to be similar to the skin lesions, with thrombi deposited in the venules.4 In 1948, Degos changed the name of the disease to papulose atrophiante maligne or malignant atrophic papulosis.19
Incidence & Prevalence
Approximately 200 cases have been reported in the literature. However, it is thought that many cases go unreported. Most patients are Caucasian, with a peak incidence in the third decade of life, but there are a few reports in children. There is a 3:1 male–female ratio.11,20,21 The cutaneous form of the disease is mostly seen in women.22 Familial forms have also been described.23
Histopathology
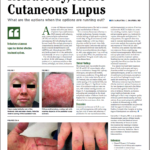
The skin lesions range from 0.3–1.0 cm in size and appear as pink to brown papules with an atrophic, porcelain-white center and erythematous, telangiectatic/violaceous border/rim.24,25 Lesions look similar in all organs.26,27 The classic histopathological findings consist of wedge-shaped infarctions with collagen degradation, endothelial proliferation and occlusion by thrombi.25 Early lesions can have perivascular inflammatory infiltrates with interstitial mucin deposition.5 There may be swelling and proliferation of endothelial cells beneath the zones of necrobiosis.5 Histologically, there is no difference in the histopathology of lesions in those with limited (cutaneous only) or the systemic form of the disease.11
Transformation from cutaneous to systemic MAP can occur within months to years following the onset of dermatologic manifestations. Systemic MAP involves small- & medium-size arteries.
Prior Medical Treatment
Multiple medication regimens had been suggested, although none was found to be effective. These include IVIG, ASA, dipyridamole, warfarin, heparin, azathioprine, tacrolimus, cyclophosphamide, bevacizumab and infliximab.28-31
Eculizumab
Eculizumab is a humanized monoclonal antibody that binds to human C5 complement protein and inhibits cleavage to C5a and C5b. This inhibition prevents both generation of the membrane attack complex (MAC) and the proinflammatory effects of C5a. Additionally, eculizumab has potent antianaphylatoxin and antichemotaxin effects. Patients should receive meningococcal vaccination at least two weeks prior to treatment.5,34
Treprostinil
Treprostinil is a long-acting prostacyclin analog that may help heal ischemic wounds and decrease pain due to ischemia; it also has some antiplatelet effects and may increase the number and angiogenic potential of endothelial progenitor cells.36,38 It had previously been observed that a patient with systemic sclerosis treated with treprostinil noted improvement of her MAP lesions.
The most common cause of death is sepsis due to peritonitis & perforation, developing within two to three years of internal organ involvement.
Lessons Learned
MAP is a rare, life-threatening disease. With the most current findings and investigations, we may be able to bring some hope to patients—or at least open the door for further investigation. Our first patient has survived four years to date with the current treatment. While on this dual therapy, he has developed atrial fibrillation and undergone cardiac ablation and, more recently, has had recurrent pleural effusion.